Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
Let me be completely honest with you about something. When patients come to me after months — sometimes years — of back pain, they are often carrying a weight far beyond the physical. The frustration of being told "your MRI shows a disc bulge" followed by a shrug, or the anxiety of a surgeon suggesting spinal fusion, or the quiet desperation of someone who has tried physiotherapy, painkillers, and rest with little relief. I see it every week across both our clinics. And it matters to me enormously.
So when I recommend intradiscal ozone therapy, it is not because it is fashionable. It is because, in carefully selected patients, I have watched this treatment transform lives — people returning to their families, their work, their morning walks — without a single incision. This article is my attempt to explain, properly, what ozone is, what it does inside a diseased disc, where the evidence sits, and precisely how we deliver it at IBAP Clinics with the caution and precision the procedure demands.
Ozone — written chemically as O₃ — is simply a molecule made of three oxygen atoms instead of the usual two. We breathe O₂ every moment of our lives; O₃ is the same element rearranged, and that rearrangement makes it extraordinarily reactive. In nature, it forms in the upper atmosphere where it shields us from ultraviolet radiation. In a clinical setting, we generate it fresh on-demand from medical-grade pure oxygen, using a precisely calibrated ozone generator — a device that applies a controlled electrical discharge to split O₂ and reassemble it as O₃.
Because ozone cannot be stored or transported, every clinical procedure uses freshly generated gas. This is not a vial sitting on a shelf. The concentration — measured in micrograms per millilitre (µg/ml) — is set immediately before injection, and this is where expertise matters enormously. The wrong concentration at the wrong site does not simply "not work". It can harm. Which is precisely why I am cautious when I hear of ozone being administered casually, without proper equipment, training, or monitoring. That caution, I would argue, is the non-negotiable foundation of everything we do at IBAP Clinics.
Ozone is not a drug in the conventional sense — it is a biologically active gas that harnesses the body's own oxidative and anti-inflammatory pathways. Its inability to be patented has slowed regulatory approval in some countries, but the clinical evidence from Europe, India, and Asia has been accumulating steadily for over three decades.

To understand how ozone works, we need to understand why the disc hurts in the first place. The nucleus pulposus — the gel-like centre of an intervertebral disc — is a remarkable structure. Think of it as a tightly packed sponge containing large hydrophilic (water-loving) proteins called proteoglycans. These proteins hold water within the disc, giving it height and the ability to absorb spinal loading. When a disc herniates or degenerates, several things happen simultaneously — and each of them feeds the other in a vicious cycle.
Discs have very poor blood supply under normal conditions. When they degenerate, local oxygen delivery falls further, creating a state of anoxia — oxygen starvation — within the disc and surrounding tissues. Anoxic tissues produce lactic acid, which stimulates pain-sensitive nerve endings. Nearby muscles respond by going into protective spasm, which compresses blood vessels further, worsening the anoxia. Meanwhile, the damaged disc releases phospholipase A₂ (PLA₂) and other inflammatory enzymes that directly sensitise nerve roots. Prostaglandins, cytokines, and substance P flood the area. The nerve root swells. The pain intensifies. This is not a simple mechanical problem — it is a biochemical fire.
When ozone (O₃) is introduced into this environment, it immediately decomposes and releases a reactive oxygen species (ROS) — a highly energetic free radical. This ROS does three things with clinical relevance:
Imagine the disc nucleus as an overfilled sponge compressed against a nerve. The sponge holds its shape because of proteins that act like tiny water-magnets. Ozone is like a very precise chemical solvent — it deactivates those water-magnets, the sponge loses water, shrinks, and the nerve is released. But unlike surgery, which physically cuts the sponge away, ozone does this from within the molecular structure of the disc itself, without disturbing the surrounding architecture. That elegance is precisely why, in appropriate cases, I prefer it over both prolonged medication and the risks of open surgery.
One of the most important concepts in ozone therapy — and one that is frequently misunderstood — is that ozone is not a "more is better" treatment. Different concentrations produce fundamentally different biological effects, and matching the concentration to the clinical target is where expertise separates good practice from dangerous practice.
| Concentration (µg/ml) | Primary Effect | Clinical Application |
|---|---|---|
| 5–15 µg/ml | Immune modulation; mild oxidative stimulus; cellular activation | Systemic ozone therapy; immune conditions; chronic fatigue |
| 15–25 µg/ml | Anti-inflammatory; tissue repair stimulation; improved microcirculation | Paravertebral injections; trigger point therapy; soft tissue pain |
| 27–30 µg/ml | Proteoglycan oxidation (nucleolysis); marked anti-inflammatory | Intradiscal — the window used at IBAP Clinics |
| 30–40 µg/ml | Strong oxidative — used in joint spaces for cartilage modulation | Intra-articular injections (knee, hip, shoulder) |
| >40 µg/ml | Risk of oxidative tissue damage — NOT used therapeutically at safe clinical practice | Not recommended for injection |
Ozone therapy in pain medicine is not a single technique — it is a family of techniques, each tailored to the tissue being treated and the pain mechanism being targeted. Understanding this is important because patients sometimes come having read about "ozone therapy" without realising that what is appropriate for a knee joint is entirely different from what is delivered into a spinal disc.
Low-concentration ozone gas used around wounds, diabetic foot ulcers, or skin infections. Not absorbed systemically. Safe, adjunctive use.
Injected into paraspinal muscles, trigger points, or gluteal musculature. Medium concentrations; relieves muscle spasm and localised inflammation.
Injected into synovial joints — knee, hip, shoulder, facet joints. Reduces synovial inflammation; useful in early osteoarthritis and degenerative joint conditions.
Injected alongside the spine or into the epidural space to reduce nerve root inflammation without entering the disc itself. Often combined with intradiscal ozone.
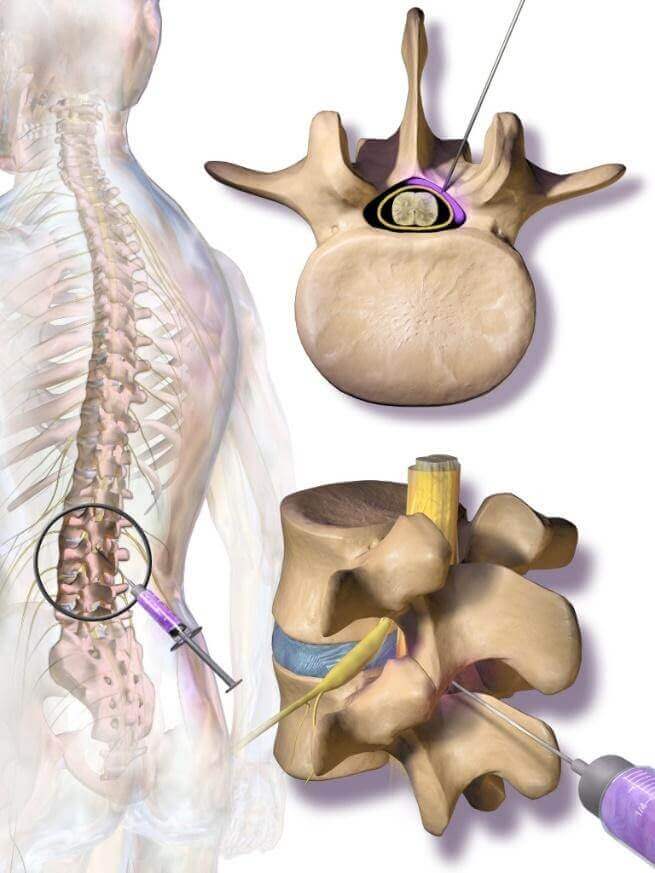
The most specialised application. Needle placed directly into the nucleus pulposus under X-ray guidance. High concentration, precise volume. Requires specialist expertise.
Patient's blood mixed with ozone outside the body and returned intravenously. Used for systemic conditions, not primarily spine pain. Separate risk-benefit assessment required.
I want to address this section with the balance it deserves. Ozone nucleolysis is not experimental in the sense of being untested — there is a substantial body of clinical evidence, including randomised controlled trials, large prospective series, and systematic reviews. What it lacks, in certain jurisdictions, is regulatory approval — and these are not the same thing.
| Study / Source | Design | Finding |
|---|---|---|
| Bonetti et al., 2005 — AJNR | RCT — 159 patients | Intradiscal + paravertebral ozone: significantly superior to steroid injection alone in lumbar disc herniation at 6 months |
| Andreula et al., 2003 — AJNR | Prospective series — 600 patients | 78.4% good-to-excellent outcome; paravertebral + intradiscal ozone vs steroid — ozone superior at all time points |
| Muto et al., 2008 — Neuroradiology | Systematic review | Endorsed ozone nucleolysis as a minimally invasive option bridging conservative and surgical treatment; favourable safety profile |
| Zhang et al., 2013 — Pain Physician | Meta-analysis | Ozone + steroid combination superior to steroid alone for lumbar disc herniation at 3 and 6 months; NRS pain reduction statistically significant |
| Gautam et al., 2011 — J Neuroradiol | Prospective RCT | Intradiscal ozone showed 80% success at 6 months compared with 48.3% for steroid alone |
| Steppan et al., 2010 — Spine J | Review of 8,000 patients across Italy | Complication rate <0.1%; no long-term adverse outcomes; recommended for contained disc herniations |
The majority of high-quality evidence comes from Italy, where ozone nucleolysis has been practised and refined since the 1980s — with tens of thousands of procedures performed under rigorous standards. China, Brazil, Spain, Colombia, and increasingly India have added their own substantial clinical experience to this body of literature.
The United States FDA and the UK MHRA classify ozone as a drug — which means it requires the same regulatory pathway as a pharmaceutical compound. The critical issue is this: ozone cannot be patented. It is a naturally occurring molecule. With no prospect of exclusive intellectual property rights, pharmaceutical companies have no financial incentive to fund the enormous randomised clinical trials required for regulatory approval — which can cost hundreds of millions of dollars. The result is a regulatory gap: not because the treatment is unsafe, but because the economic model for approval does not exist. Physicians in these countries who use ozone are not breaking any law, but they operate outside the standard of care framework, which creates significant medicolegal exposure. Clinical practice in countries such as Italy, where ozone nucleolysis is formally recognised and reimbursed, has consequently advanced far beyond where the anglophone regulatory environment sits.
I have performed many thousands of ozone procedures across my career — first in the United Kingdom, where I trained at some of the most demanding pain medicine programmes in the world, and subsequently here in Hyderabad where I established IBAP Clinics. Every single procedure I do is conducted with a level of care that I would want applied to a member of my own family. Not as a marketing claim. As a clinical standard.
Let me walk you through exactly what happens when a patient comes to us for intradiscal ozone.
Not every back pain patient is a candidate for ozone nucleolysis. We review the MRI carefully — ideally a recent study not older than six months. Contained disc herniations respond best. Severely degenerated discs with loss of disc height, frank extrusions, or sequestered fragments may require different management. Patients with active infection, coagulopathy, uncontrolled diabetes, or certain immune conditions are not treated with intradiscal ozone. The time I spend at consultation is not a formality. It is the most important part of the procedure.
We use medical-grade oxygen and a certified ozone generator. Concentrations are set specifically for the target — typically 27–30 µg/ml for intradiscal injection and 15–20 µg/ml for paravertebral injection administered in the same session. These figures are not approximations. They are precise, reproducible, and documented in every patient record.
The needle does not go anywhere without live fluoroscopic X-ray confirmation. We confirm the correct disc level. We confirm correct needle position within the nucleus. A small volume of contrast confirms needle placement before a single millilitre of ozone is introduced. There is no "feel" technique for intradiscal work — there is only imaging confirmation. Full stop.
Throughout the procedure, the patient's heart rate, blood pressure, and oxygen saturations are monitored continuously. We have full resuscitation equipment available. Post-procedure, patients rest in recovery before discharge.
At IBAP Clinics, we typically combine intradiscal ozone with paravertebral ozone injection — directly alongside the inflamed nerve root. This combined approach addresses both the mechanical (disc herniation) and neurochemical (nerve root inflammation) components of the problem simultaneously, and our outcomes reflect this comprehensive approach.
In my experience with many thousands of cases, the results have been consistently excellent for well-selected patients. Patients who have been told their only option is surgery frequently discover that they can recover function, return to work, and live without daily pain — without a single incision.
| Feature | Intradiscal Ozone | Epidural Steroid | Laser Disc Decompression | Surgery (Discectomy) |
|---|---|---|---|---|
| Targets disc structure directly | ✔ | ✘ | ✔ | ✔ |
| Anti-inflammatory action | ✔ | ✔ | ✘ | ✘ |
| Repeatable | ✔ | Limited | ✘ | ✘ |
| General anaesthetic required | ✘ | ✘ | ✘ | ✔ |
| Hospital admission | ✘ | ✘ | ✘ | ✔ |
| Risk of post-operative complications | Minimal | Minimal | Low | Significant |
| Evidence grade (disc herniation) | Level I–II | Level I | Level II–III | Level I |
Over the years, a pattern has emerged in my practice that I cannot ignore. The patients coming through our doors at Banjara Hills and Madeenaguda have changed. Fifteen years ago, the typical disc pain patient was middle-aged, a manual worker, someone who had lifted something heavy or taken a fall. Today — and I say this not as a criticism but as an observation — I am seeing software engineers in their late twenties, data analysts who sit eight to ten hours daily, young professionals commuting long distances on poor roads in Hyderabad traffic, and more recently, students. Yes, students. Young people whose backs should not yet be speaking the language of pain.
India's extraordinary economic growth has brought with it an epidemic of sedentary living. The IT corridors of Hyderabad — HITEC City, Gachibowli, Madhapur — are full of brilliant young people hunched over screens in postures their spines were never designed for. And unlike a decade ago, there is enormous pressure not to rest. Deadlines do not pause for back pain. Managers are not always sympathetic. The culture of powering through, of dismissing one's own pain as weakness, runs deep. I have had patients admit they delayed coming to see me for two years because they thought the pain would "settle on its own."
It often does not settle. It often gets worse. And when disc pathology is caught early — when the herniation is still contained, when the nerve root inflammation has not become chronic — that is precisely when intradiscal ozone produces its most dramatic results. Which is why I feel strongly: if you are living with back pain that is limiting your function, please do not wait.
Pain is not a personality flaw. I have sat across from enough engineers, executives, and young professionals in Hyderabad to know that this city runs on people who have been conditioned to dismiss their own discomfort. But the disc does not care how dedicated you are. It responds to physics and biology, not willpower. My job is not just to treat the disc — it is to validate what you are feeling, explain it clearly, and offer you a path forward that does not involve accepting chronic pain as your new normal. Empathy, in my view, is not the soft part of medicine. It is the foundation upon which good clinical decisions are made.
Book a specialist consultation with Dr. Vijay Bhaskar Bandikatla. We will review your MRI, discuss your history, and give you an honest, evidence-based opinion on whether ozone nucleolysis is appropriate for your specific disc problem.
2nd Floor, 284/A, Road No. 12
Above IDFC First Bank
Near Omega Hospitals, MLA Colony
Banjara Hills, Hyderabad 500034
Sy No. 2, 4th Floor, Plot No. 200
Beside South India Shopping Mall
Opp. Fortune Heights, Mythri Nagar
Madeenaguda, Hyderabad 500049
This article has been written by Dr. Vijay Bhaskar Bandikatla (MBBS, DA, FRCA, FFPMRCA, CCT UK) for general educational purposes only. The information presented does not constitute medical advice and must not be used as a substitute for a formal consultation with a qualified pain medicine specialist. Intradiscal ozone therapy is a specialist procedure that requires individual patient assessment, review of diagnostic imaging, and clinical judgement by an appropriately trained practitioner. Treatment suitability varies between individuals. Results described are based on clinical experience and published literature and may not apply to all patients. If you are experiencing back or neck pain, please consult a qualified medical professional. IBAP Clinics — Indo British Advanced Pain Clinics, Hyderabad — Vijay Advanced Pain Clinics Pvt. Ltd.


