Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
Most sciatica does not need surgery. Accurate diagnosis, expert intervention and disease arrest can transform outcomes without the risks and consequences of an operation.

Sciatica Key Takeaways at a Glance
Sciatica is a painful nerve condition usually caused by a bulging disc, but it rarely requires surgery. IBAP Clinics advocates for minimally invasive, non-surgical treatments like targeted injections and regenerative therapies to calm inflammation and heal the disc naturally, reserving surgery only for rare medical emergencies.
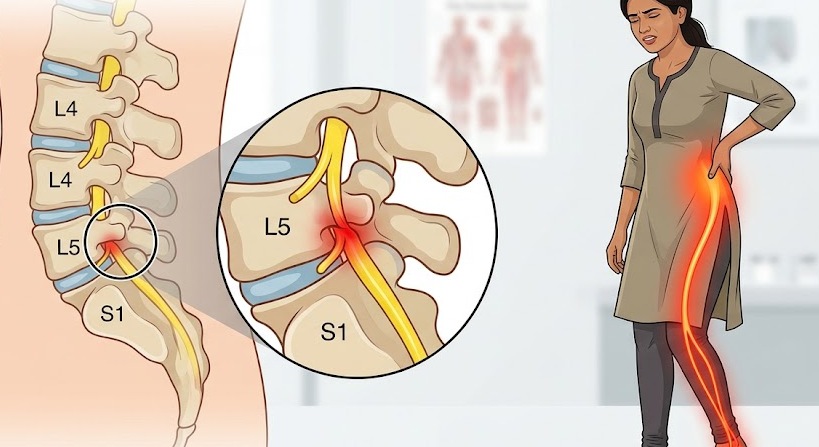
Sciatica is not a diagnosis in itself it is a symptom. It describes pain, numbness, tingling, or weakness that travels along the path of the sciatic nerve: from the lower back, through the buttock, down the back of the leg, and sometimes all the way to the foot.
Think of the sciatic nerve as the body’s longest electrical cable roughly the width of your thumb at its origin, branching from five nerve roots in the lower spine (L4, L5, S1, S2, S3). When any part of that cable is compressed, inflamed, or irritated, signals misfire, creating the characteristic shooting, burning, or electric-shock sensation that patients describe.
The condition affects an estimated 10–40% of the population at some point in their lives and is one of the most common reasons people seek pain specialist care. Yet it remains one of the most over-treated conditions in medicine, with surgery offered far more frequently than the evidence justifies.

The sciatic nerve roots emerge through small bony windows called intervertebral foramina. Any condition reducing the space available for those nerves inside the canal or at the exit point can trigger sciatica. The most common causes are:

The intervertebral disc acts like a shock-absorbing cushion between each pair of vertebrae. Its outer layer the annulus fibrosus is a tough fibrous ring. Inside is the nucleus pulposus, a gel-like core. When the annulus develops cracks (annular tears) or weakens, the nucleus can bulge outward or rupture through the outer wall entirely. This displaced material directly presses on a nearby nerve root the mechanical equivalent of stepping on an electrical cable. Even without direct contact, leaked disc material triggers a potent inflammatory chemical cascade that irritates the nerve.

Stenosis means narrowing. The central spinal canal can narrow due to thickened ligaments, arthritic facet joint overgrowth, or disc bulging. More common in the over-50 population, it produces the hallmark symptom of neurogenic claudication: leg pain worsened by standing/walking, relieved by sitting forward.

The intervertebral foramen is the exit tunnel for each nerve root. Narrowing here from disc height loss, facet joint arthritis, or bone spurs is like a wire pinched at a cable gland, producing pain precisely in the territory of that specific nerve.
One vertebra slips forward over the one below it like a brick overhanging another. This creates foraminal narrowing on both sides and, in more severe cases, central canal compression. It may be degenerative (wear and tear), isthmic (stress fracture, common in young athletes), or traumatic.
CLINICAL NOTE
Multiple causes can coexist. A patient may have a disc bulge at L4-L5 AND foraminal stenosis at L5-S1. Careful clinical examination and targeted imaging are needed to identify the dominant pain generator one of the key skills in interventional pain medicine.
Understanding the pathway from a disc problem to leg pain helps demystify sciatica. It is a sequence, not a single event:
1, Annular Tear: The outer ring of the disc develops a crack from repetitive loading, poor posture, or a sudden twist. This may initially cause local low back pain a deep ache worse on sitting.
2, Inflammatory Response: The tear allows inflammatory chemicals (TNF-α, interleukins, phospholipase A2) to leak from inside the disc. These are highly irritating to nearby pain-sensitive structures, explaining why discogenic back pain can be severe even without nerve compression.
3, Disc Material Leaks into the Canal or Foramen: If the annular tear progresses, nuclear material herniates into the spinal canal or foramen. Sciatica truly begins: the nerve is now both mechanically compressed and chemically bathed in inflammatory mediators.
4, Nerve Root Irritation and Radiculopathy: The irritated nerve root becomes hypersensitive and swollen. Signals distort, producing shooting pain, pins and needles, numbness, and in advanced cases, muscle weakness.
5, Chronification: If the nerve remains inflamed over weeks/months, central sensitisation develops — the spinal cord and brain become amplifiers of pain. Early, accurate intervention matters: arresting the disease process before it becomes entrenched protects long-term function.
Diagnosis is clinical first imaging second. A skilled pain physician performs a detailed neurological examination: reflexes (ankle jerk for S1, knee jerk for L4), muscle power testing, and dermatomal sensation mapping. This points to the likely nerve level before any scan.
MRI of the lumbar spine remains the gold standard investigation, demonstrating disc morphology, nerve root compression, and canal dimensions. CT myelography is occasionally used when MRI is contraindicated or to plan precision procedures.
IMPORTANT: DO NOT OVER-INTERPRET MRI
Studies show that disc bulges are visible on MRI in up to 50% of people over 40 who have NO back pain at all. An MRI finding must always be correlated with clinical symptoms and signs. Treating an MRI report rather than a patient is one of the most common causes of unnecessary surgery.
“Only 1 to 2 percent of all back pain truly requires surgical intervention. Many surgeries that are done could have been avoided with proper expertise, thoughtful planning, and a timely second opinion. Too often, surgery is a decision born of desperation — the patient’s and sometimes the surgeon’s.”
— Dr. Vijay Bhaskar Bandikatla, FRCA FFPMRCA | Advanced Pain Consultant, IBAP Clinics, Hyderabad
The natural history of sciatica due to disc herniation is, in most cases, favourable. The disc material that herniates is gradually reabsorbed by the body’s immune system over weeks to months a process called spontaneous regression. Studies using serial MRI scans have shown significant or complete regression in 60–80% of disc herniations without surgery.
The problem is that this natural recovery can be painful and slow. Waiting without treatment is not the answer but waiting without surgery specifically is usually perfectly reasonable. The correct approach is targeted interventional pain management: relieving the nerve of its inflammatory burden, reducing chemical irritation, and supporting recovery through disease-modifying procedures.
WHY UNNECESSARY SURGERIES HAPPEN
The patient is in severe uncontrolled pain and feels they have no other option.
The treating clinician’s toolkit does not include advanced interventional procedures.
A second expert opinion was never sought.
At IBAP, we believe every patient considering spinal surgery deserves a thorough, honest assessment of non-surgical options first.
Minimally Invasive Percutaneous Spinal Interventional (MIPSI) procedures sit between physiotherapy and surgery on the treatment ladder. Performed under imaging guidance (fluoroscopy or CT), usually as day procedures with minimal recovery time, they target the exact pain generator with precision.
Corticosteroid delivered into the epidural space bathes inflamed nerve roots directly, rapidly suppressing the inflammatory cascade. Performed by interlaminar, caudal, or transforaminal (targeted) approaches.
Platelet-Rich Plasma and other biologic agents harness the body’s own healing signals. Injected into or around a damaged disc, PRP can promote repair of annular tears and modulate inflammation.
Radiofrequency energy reduces intradiscal pressure and ablates pain-generating nerve fibres within the disc. A disc preservation strategy that reduces symptoms while maintaining disc structure.
For sciatica from vertebral compression fractures (osteoporotic or oncological), vertebroplasty stabilises the collapsed vertebra and relieves pain, often within hours.
Highly targeted injection delivered to the exact nerve root involved. Both diagnostic (confirms which nerve is the source) and therapeutic. Particularly valuable when one specific level is responsible.
Treatment of the disc from within under fluoroscopic guidance including intradiscal steroid injection, electrothermal therapy (IDET), and radiofrequency-based disc ablation.
Modulates nerve pain transmission without destroying the nerve. Applied to a dorsal root ganglion, PRF ‘resets’ the sensitised nerve, providing relief lasting months to years.
For persistent sciatica and failed back surgery syndrome, neuromodulation through an implanted SCS can transform quality of life. IBAP has expertise in SCS implantation and programming.
A disc removed is a disc gone forever. The intervertebral disc is a biomechanical marvel shock absorber, motion segment, and spacer that keeps the foramen open for the nerve. Once removed or fused, adjacent segments must compensate with extra loading, accelerating adjacent-level disease. This is the “cascade” that leads patients back for second, third, and fourth surgeries.
At IBAP, our priority is to treat the disc as a living structure to be preserved and rehabilitated where possible. Our disc preservation toolkit includes:
DISEASE ARREST, NOT JUST PAIN RELIEF
The goal of IBAP disc interventions is not merely temporary pain relief. By treating the underlying disc pathology the annular tear, the chemical inflammation, the nuclear degeneration we aim to arrest disease progression and give the disc the best chance of healing. Think of it as conserving a damaged building rather than demolishing and rebuilding it.
When patients come to Indo British Advanced Pain Clinics whether referred for a second opinion before surgery or in the early stages of their sciatica journey they receive an honest assessment of all options, including the option of not proceeding with any intervention.
Dr. Vijay Bhaskar Bandikatla trained in Advanced Pain Medicine at Cambridge and completed his Pain Fellowship in London, with additional training across Europe and the USA. He holds a Diploma in Sports Medicine (DDSMed, ISST Pune, recognised by ISPA Chicago) and an MBA in Hospital Management. The approach at IBAP is genuinely multidisciplinary.
Our promise to every patient includes:
Intellectual honesty demands acknowledgement: there are circumstances where spinal surgery is not just appropriate but urgently necessary. These are relatively rare, but when they apply, delay is dangerous.
EMERGENCY — SEEK IMMEDIATE HOSPITAL ATTENDANCE FOR:
Cauda Equina Syndrome: sudden loss of bladder or bowel control, saddle anaesthesia (numbness in inner thighs/perineum), or rapidly progressive bilateral leg weakness. This is a spinal emergency requiring surgical decompression within hours. Do not delay.
Beyond emergencies, surgery is a reasonable and well-evidenced choice when:
Start your journey with a virtual consultation to discuss symptoms from home.
We review your medical history and relevant reports for a clear understanding.
Our doctors conduct a thorough assessment through detailed discussions.
We confirm findings with state-of-the-art imaging like X-rays, CT scans, and MRIs.
Our team identifies the root cause and key trigger points for treatment.
We create a customized treatment plan, including necessary medications and procedures.
Our Pain Specialists support a complete recovery focused on total wellness.
We provide ongoing follow-ups tailored to each treatment plan, ensuring continuous care and long-term recovery support.
We relieve your pain, helping you be yourself again!
Sciatica is a nerve pain condition where sharp, shooting pain travels along the sciatic nerve. The pain usually starts from the lower back, passes through the hips, and moves down one or both legs.
Sciatica usually occurs when the sciatic nerve is compressed or irritated. Common causes include a herniated disc, spinal stenosis, bone spur, or other spinal conditions that put pressure on the nerve roots.
Sciatica pain is often described as sharp, shooting, burning, or electric-shock-like pain. It may worsen with sudden movements, prolonged sitting, bending, or standing for long periods.
Common symptoms include lower back pain, hip pain, leg pain, numbness, tingling, weakness, and discomfort that travels down the leg. In some cases, the pain can make walking or daily activities difficult.
Yes. Many cases of sciatica can be managed with non-surgical treatment such as spinal decompression therapy, targeted physical rehabilitation, posture correction, pain management, and guided exercises.
IBAP Clinics offers spinal decompression therapy, targeted physical rehabilitation, precision injections, and minimally invasive consultation when required. The treatment plan is tailored according to the patient’s condition and pain severity.

EXCELLENTTrustindex verifies that the original source of the review is Google. Good pain relief with treatmentPosted on GoogleTrustindex verifies that the original source of the review is Google. Best for pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. बहुत अच्छा लगा हमें ये ट्रिटमेंट करा के अच्छे डॉक्टर और अच्छे स्टाफ हैं और काम पैसे में अच्छा अच्छा ट्रिटमेंट होता हैPosted on GoogleTrustindex verifies that the original source of the review is Google. Very nice, good and helpful staf, overall good experiencePosted on GoogleTrustindex verifies that the original source of the review is Google. Very good doctors and good tritment Thank you doctorPosted on GoogleTrustindex verifies that the original source of the review is Google. One of the best clinic for the relief of back painPosted on GoogleTrustindex verifies that the original source of the review is Google. Very good treatment indo british clinic for every pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. I have visited indo british pain clinic this is superb clinic for pain relief that's why I have given 5 start rating to this clinic ...Posted on GoogleTrustindex verifies that the original source of the review is Google. My name is Raja Sekhar Reddy Tummuri from kakinada city My father was suffering nervous pain from last 3 years … I have decided to join with this op … Now everything fine after treatment done from DR. vijay sir … Wonderful service received from INDO British advanced pain clinic Hospitals in Hyderabad @ Banjara Hills road no 12.. Each and every staff response , concern , support & everything it’s too good Thank you so much … Special thanks to Mr. DR. Vijay bhaskar Bandi Katla …👏🏻👏🏻👏🏻👏🏻🙏🙏Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
Medical Disclaimer: This article is written for patient education by a qualified pain medicine specialist and reflects evidence-based clinical practice. It is not a substitute for a personalised medical consultation. Emergency symptoms (bladder/bowel dysfunction, rapidly worsening weakness) require immediate hospital attendance.

MBBS, DA, FRCA (UK), FFPMRCA (Pain Medicine, RCOA, UK)
CCT (Anesthesiology And Pain Management)
Neuromodulation & Advanced Pain Research Fellowship (London), MBA (HM)
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us