Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
Cancer pain is one of medicine’s most devastating and yet most treatable challenges. Uncontrolled pain does not just hurt – it steals a patient’s will to fight, isolates families, and derails treatment. At IBAP Clinics, Hyderabad, we believe that managing your pain is not separate from fighting your cancer. It is part of the fight.


Imagine you are in the middle of a war – fighting for your life against cancer. Now imagine that battle being fought with a broken leg, untreated. Every step, every movement, every attempt to rest is accompanied by relentless, consuming pain. That is the daily reality for millions of cancer patients in India whose pain is not adequately managed.
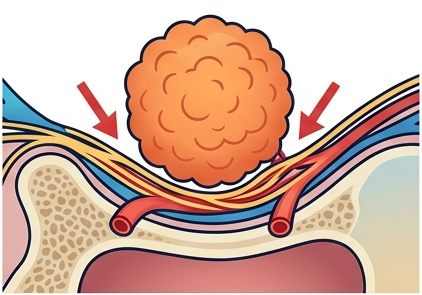
Cancer pain is not a single, uniform experience. It is a complex, shifting composite of multiple pain mechanisms firing simultaneously a tumour pressing on a nerve, an eroded rib, chemotherapy scorching the nerve endings in both hands, radiation fibrosing the lung tissue. Unlike the clean, linear pain of a sports injury, cancer pain evolves, intensifies, and spreads as the disease progresses often faster than oral medications alone can track.
A landmark 2016 meta-analysis published in The Journal of Pain and Symptom Management found that 55% of patients undergoing anti-cancer treatment experience pain, rising to nearly 70% in advanced or metastatic disease. And in a finding that should shame every healthcare system, nearly half of all cancer patients globally receive inadequate analgesia.

In India, the picture is even starker — as we shall examine in the following section. But let us be clear from the outset: the tools to relieve cancer pain effectively exist. They exist right here at IBAP Clinics in Hyderabad. The challenge is ensuring that every patient who needs them reaches a specialist who can deploy them.
Pain control is not a comfort measure added after cancer treatment it is an integral component of cancer treatment itself. A patient in uncontrolled pain cannot sleep, eat, maintain immunity, tolerate chemotherapy, or engage meaningfully with their loved ones. Treating the pain is treating the whole patient.
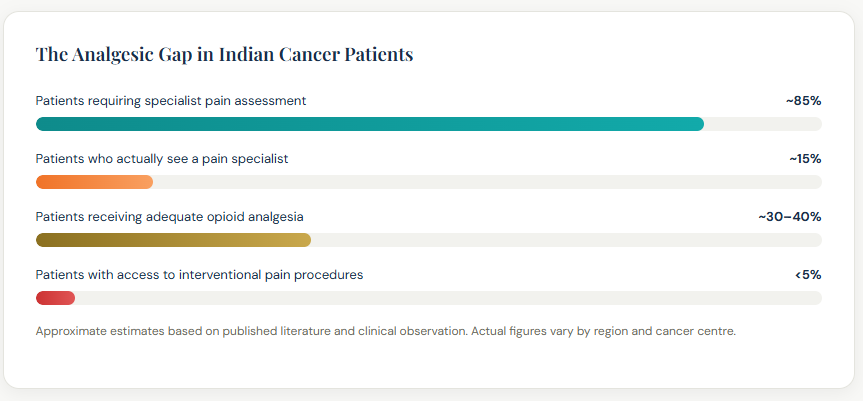
India’s cancer pain crisis is a story of multiple compounding failures of awareness, of access, of stigma, and of a healthcare system where pain specialists are bypassed in the rush from oncologist to hospital, and back again. Consider this: India accounts for nearly 8% of global cancer deaths, yet consumes less than 1% of the world’s medical morphine. That gap is not a reflection of less pain it is a reflection of how catastrophically undertreated that pain is.
In India, the typical cancer patient’s journey looks like this: diagnosis at a government hospital or private oncology centre → chemotherapy or radiation → oncologist follow-up. At no point in this pathway is a pain specialist routinely consulted even when the patient’s pain is severe, or when opioid side effects have become intolerable.
Think of it like this: if your car’s engine is on fire, you go to an engine specialist not the salesperson who sold you the car. Yet Indian cancer patients are being managed for complex, multi-mechanism pain by oncologists whose primary expertise is tumour biology and cytotoxic treatment. No criticism of oncologists is intended they are exceptional at what they do. But pain medicine is a specialist discipline in its own right, requiring its own set of skills and tools.
The reasons behind this gap are multiple and interconnected:
💡 An Indian Reality — The Rameshankar Example
Consider Rameshankar, a 58-year-old farmer from Nalgonda diagnosed with pancreatic cancer. His oncologist at a district hospital prescribed tramadol, which helped initially. Six months later, he is in agony the tramadol is no longer effective, he is severely constipated from escalating codeine doses, and he has stopped eating. His family believes this is simply “how cancer ends.” Nobody told them that a neurolytic coeliac plexus block a single, day-procedure intervention could relieve his pain for months with minimal side effects. This is the gap that IBAP Clinics exists to close.
Understanding why cancer hurts is the essential first step to treating it effectively. Cancer pain is not one problem it is a building with six different entry points, each requiring its own specialist key.

In clinical practice, most cancer patients experience mixed-mechanism pain — nociceptive, inflammatory, and neuropathic components simultaneously. This is why a single drug class rarely provides complete relief, and why a multimodal approach combining medications, adjuvants, and targeted interventional procedures is the gold standard.
Radiation therapy is a cornerstone of cancer treatment but it carries a long-term consequence that is insufficiently recognised, even within oncology: radiation-induced fibrosis.
Think of healthy tissue as a well-organised fabric flexible, strong, with each thread in its proper place. Radiation damages the connective tissue framework of this fabric. In response, the body lays down scar tissue fibrous, inelastic, and poorly vascularised. Over weeks, months, and sometimes years after radiation therapy, this fibrotic tissue contracts, tightens, and critically entangles and entraps the nerves, blood vessels, lymphatics, and muscles running through the treated area.
The result is radiation fibrosis syndrome a progressive, often painful and debilitating condition that can emerge long after the cancer itself is under control. Many patients and clinicians mistakenly attribute this pain to cancer recurrence, causing additional anxiety and unnecessary investigation.
Radiation fibrosis pain typically develops months to years after treatment ends, long after the patient has been discharged from active oncology follow-up. Many patients with post-radiation neuropathic pain are told “there is nothing more to be done” — yet targeted interventions including nerve blocks, physiotherapy, hyperbaric oxygen, and neuromodulation can significantly improve function and reduce pain. Early referral to a pain specialist is essential.
There is a dangerous and widely held assumption that once cancer is in remission, the pain disappears with it. For a significant proportion of cancer survivors worldwide and in India, where millions have completed treatment this assumption is cruelly wrong.
If a storm damages a building, the storm passing does not automatically repair the walls. Similarly, the neural, muscular, and connective tissue damage inflicted by cancer and its treatments can persist for years or permanently after the cancer has been treated. Survivors often feel guilty acknowledging ongoing pain when they have “beaten cancer” yet their suffering is real, and it is treatable.
Common chronic pain syndromes in cancer survivors include post-mastectomy pain syndrome, chemotherapy-induced peripheral neuropathy, radiation fibrosis and plexopathy, lymphoedema, hormone-therapy-induced musculoskeletal pain, and entirely unrelated age-related conditions such as osteoarthritis and disc disease that deserve their own assessment and treatment.
India has an estimated 3–5 million cancer survivors — a number growing rapidly with improving treatment outcomes. The majority have ongoing pain that is undertreated. A dedicated cancer survivor pain assessment at IBAP Clinics can provide these patients with the specialist attention they deserve.
Untreated cancer pain is not merely an inconvenience. It unravels the entire human system — physically, psychologically, and socially — undermining the very capacity to fight the cancer that caused the pain in the first place.
When cancer pain is managed only by escalating oral opioids without adjuvants, nerve blocks, or specialist titration the medication itself becomes a source of suffering:
Imagine you have been in severe, unremitting pain for six months. Every morning you wake up not refreshed, but exhausted because sleep was shattered by breakthrough pain. Every meal reminds you of how little you can eat because the pain, and the side effects of the medications trying to manage it, have destroyed your appetite. Every visit to the hospital feels not like a step towards recovery, but another ordeal to endure.
At some point and this point comes sooner than anyone admits patients stop believing the fight is worth it. They decline the next cycle of chemotherapy. They do not attend their radiation appointment. They refuse the surgical procedure that might have extended their life. Not because they have accepted death, but because the pain has made living feel worse than the alternative.
This is not weakness. This is a physiological and psychological response to sustained, undertreated suffering. And it is preventable.
At IBAP Clinics, we have seen patients who had “given up” who had told their oncologist they would not continue treatment regain hope, re-engage with their care team, and resume treatment within days of a well-executed pain intervention. A coeliac plexus block for a man with pancreatic cancer who could not eat because of abdominal pain. An epidural catheter for a woman with cervical cancer who was bed-bound from pelvic pain. The pain was managed. The person returned. The fight resumed.
Pain management is not an afterthought to cancer treatment. It is what makes cancer treatment possible and what gives patients the strength, clarity, and will to keep going.
In palliative and supportive oncology, the goals of pain management are fundamentally different from routine chronic pain care. The framing shifts from “eliminating the source” to “maximising the quality and meaning of the time available.”
We believe that every cancer patient deserves to spend their time however much of it they have doing the things that matter to them, with the people they love. Not restricted to a bed, not sedated into passivity, not in unnecessary pain. Our role is to make that possible.
Step 1 — Non-Opioid Analgesics Adjuvants
For mild pain (NRS 1–3). Always combine with adjuvants targeting the specific pain mechanism. These drugs should be continued at all higher steps.
For mild-to-moderate pain (NRS 4–6). Many Indian patients are undertreated at this step or kept here when Step 3 is clearly indicated. Low-dose oral morphine is increasingly recommended instead of codeine.
For moderate-to-severe pain (NRS 7–10). This step is critically underused in India. Strong opioids used appropriately in cancer pain do not cause addiction — they restore function and dignity. Rotation between opioids may be necessary to optimise analgesia and reduce side effects.
When pharmacological optimisation alone is insufficient, poorly tolerated, or producing unacceptable side effects. Interventional procedures target pain at its anatomical source, dramatically reducing opioid requirements and restoring quality of life. This step is where IBAP Clinics adds unique value.
Medications remain the backbone of cancer pain management. The art lies not just in choosing the right drug, but in combining the right drugs — targeting multiple pain pathways simultaneously — and adjusting as the patient’s condition evolves.
When a patient’s pain is poorly controlled or side effects become intolerable on one opioid, switching to a different opioid molecule opioid rotation can restore analgesia. This counterintuitive strategy exploits differences in individual receptor binding and metabolic pathways. Rotating from high-dose oral morphine to transdermal fentanyl, for example, often dramatically reduces constipation and sedation whilst maintaining pain control a transformation that can feel miraculous to patients who have been suffering for months.
Cancer pain management is an evolving field. Beyond the established WHO ladder and interventional procedures, a number of newer and emerging therapeutic options are expanding the palette of relief available to patients.
Cannabinoids including THC (tetrahydrocannabinol) and CBD (cannabidiol) interact with the body’s endocannabinoid system to modulate pain, nausea, appetite, and sleep. Dronabinol (synthetic THC) and nabilone are licensed in several countries for cancer pain and chemotherapy-induced nausea. Evidence for cancer pain is promising, particularly for neuropathic and refractory pain. India’s regulatory framework for cannabis-based medicines is evolving; at IBAP Clinics we discuss all options transparently with patients and families, including those available through legitimate clinical channels.
Ketamine is an NMDA receptor antagonist used at sub-anaesthetic doses as a powerful adjuvant for opioid-refractory cancer pain and opioid-induced hyperalgesia (OIH). It acts on pathways that conventional opioids cannot reach. Administered as a short IV infusion or as a subcutaneous infusion, ketamine can “reset” central pain sensitisation, allowing opioid doses to be reduced. It is particularly useful for neuropathic cancer pain, incident pain (pain triggered by movement), and situations where opioid tolerance has rendered standard analgesics ineffective. At IBAP Clinics, ketamine infusions are available in a supervised clinical setting.
Ziconotide (intrathecal) a non-opioid calcium channel blocker derived from cone snail venom provides potent analgesia for refractory cancer pain without opioid side effects or tolerance. Tapentadol, a newer analgesic that combines mu-opioid agonism with noradrenaline reuptake inhibition, offers dual-mechanism pain relief with a reduced constipation burden compared to classical opioids. Low-dose naltrexone (LDN) is an emerging area of research for inflammatory and neuropathic cancer pain.
Anti-NGF (nerve growth factor) monoclonal antibodies such as tanezumab target the inflammatory mediator responsible for bone pain sensitisation in metastatic disease though their development has been complex due to joint safety signals. Bisphosphonate-conjugated radionuclides such as Radium-223 target bone metastases directly, reducing skeletal pain whilst also providing anti-tumour effect. These represent the emerging frontier of cancer pain pharmacology.
Not all newer agents are uniformly available across India. At IBAP Clinics, we are committed to staying at the forefront of evidence-based pain medicine and will always discuss all available and emerging options with our patients, including realistic assessment of availability, cost, and expected benefit. Our aim is always to find the most effective solution that is actually accessible to our patients.
When medications even optimally prescribed fail to adequately control cancer pain, or when their side effects undermine quality of life, interventional pain procedures offer targeted, minimally invasive techniques that interrupt pain at its anatomical source.
The analogy is simple: taking oral painkillers for cancer pain is like turning down the volume on a fire alarm while the fire keeps burning. An interventional procedure cuts the wire to the alarm at the source of the fire. The relief is more precise, longer-lasting, and allows for dramatic reductions in opioid dosage and its associated side effects.
Upper abdominal cancer pain pancreatic, gastric, hepatic, and biliary cancers
The coeliac plexus is the body’s central “relay station” for pain signals from the upper abdominal organs stomach, pancreas, liver, gallbladder, and small intestine located around the aorta just below the diaphragm. A neurolytic coeliac plexus block injects absolute alcohol or concentrated phenol under fluoroscopic or CT guidance, selectively destroying the nerve fibres transmitting this pain.
Pancreatic cancer pain is among the most severe and treatment-resistant in oncology yet NCPB provides significant relief in 70–90% of patients, often transforming a patient who cannot eat or sleep from pain into one who can engage with family and tolerate their oncological treatment. The procedure is performed under sedation as a day procedure, with most patients experiencing relief within 24–48 hours.

Upper and mid-abdominal cancer pain — chemical or radiofrequency ablation
The splanchnic nerves carry pain signals from the upper abdominal organs to the coeliac plexus, travelling alongside the thoracic vertebrae (T5–T12). Targeting these nerves higher up the chain via neurolytic injection with alcohol or phenol, or via radiofrequency ablation (RFA) provides precise pain relief with several advantages over NCPB.
Splanchnic nerve ablation is particularly valuable where post-surgical anatomy or prior radiation has distorted the coeliac plexus region, and where RFA is preferable to neurolytic injection for safety reasons. Evidence shows comparable efficacy to NCPB with potentially greater durability using RFA. Applicable to pancreatic, gastric, hepatic, and upper colonic cancers.

Pelvic, gynaecological, colorectal, and prostate cancers
For visceral pelvic pain from gynaecological (cervical, ovarian, uterine), colorectal, bladder, and prostate cancers, the superior hypogastric plexus block interrupts pain signals at the pelvic nerve ganglion. For perineal pain the exquisitely distressing pain in the perianal and perineal region common in rectal and anal cancers the ganglion impar block targets the terminal sympathetic ganglion anterior to the coccyx. Both procedures are performed under fluoroscopic guidance and can provide dramatic, sustained relief for this often-inadequately managed pain location.

Tailored to pain location and mechanism
Bone metastases particularly vertebral body metastases present a dual challenge: they cause severe, often incapacitating pain, and they structurally weaken the bone to the point of collapse. A tumour eating into a thoracic vertebra is like a termite colony hollowing out a load-bearing beam the structure may hold for a while, but a minor additional stress (a cough, a turn in bed) can cause catastrophic failure.
RT is planned and delivered to shrink the tumour and weaken cancer cells within the vertebra
Imaging confirms tumour response; structural integrity assessed by specialist team
Cement augmentation performed into the RT-treated vertebra for structural reinforcement
Patient mobilises earlier; opioid weaning begins; quality of life restored
Why radiotherapy first? Radiation weakens the tumour cells and reduces vascularity of the metastasis but this very process can transiently increase the risk of vertebral collapse during the RT course. Cement augmentation after RT secures the bone that radiation has treated, preventing collapse whilst the tumour cells die and the structural benefit of RT is realised. Additionally, cement in the treated field does not significantly interfere with future radiation planning.
For patients with impending fracture or severe instability, kyphoplasty may need to precede or run concurrent with RT a decision made jointly by the interventional pain specialist and the radiation oncologist. At IBAP Clinics, we work in close liaison with oncology colleagues at Apollo Hospitals and other centres to ensure this coordination is seamless for our patients.
When medications and nerve blocks are not enough delivering analgesia precisely where it is needed, with maximum effect and minimum systemic burden.
Think of oral opioids as watering an entire garden from a helicopter the water reaches the plant, but most is dispersed everywhere else. Epidural and intrathecal drug delivery systems get the hosepipe right to the roots. By delivering analgesic medications directly into the epidural or intrathecal space adjacent to or within the cerebrospinal fluid extraordinarily small doses produce profound, targeted analgesia with dramatically fewer systemic side effects.
In Western healthcare systems, surgically implanted ITDDS pumps costing ₹8–15 lakh or more are the standard of care for refractory cancer pain. In India, this approach faces real barriers for many patients:
At IBAP Clinics, we offer an intrathecal catheter connected to an external infusion pump as a highly effective, pragmatic, and cost-accessible alternative. This provides:
We believe that the right of every patient to relief from severe cancer pain should not be determined by their bank balance. The external intrathecal catheter system bridges the gap between the ideal and the achievable and for many of our patients, it has been genuinely life-changing.
Epidural or intrathecal delivery whether via external catheter or implanted pump is considered when:
One of the most distressing aspects of severe cancer pain is helplessness waiting for a nurse to respond to a call bell, watching the clock for the next permitted dose, feeling entirely dependent on others to manage something as fundamental as your own comfort. Patient Controlled Analgesia (PCA) returns autonomy to the patient a small but profoundly important restoration of dignity and control.
PCA is a drug delivery system most commonly intravenous (IV), but also subcutaneous (SC) or, in the context of epidural and intrathecal catheters, neuraxial that allows the patient to self-administer a pre-programmed bolus dose of analgesic by pressing a button. The system incorporates lockout intervals and maximum dose limits to prevent overdose, whilst giving the patient genuine control over their moment-to-moment comfort.
Think of PCA as the difference between waiting for the waiter to bring you water when you are thirsty, and having a water jug on your own table. The autonomy is transformative particularly for cancer patients who already feel that the disease has stripped them of control over so much of their lives.
In India, subcutaneous PCA is increasingly used in palliative home care settings. A small battery-powered pump can be set up at home, with carer training provided by the pain team. For many Indian families who prefer to care for their loved one at home a deeply held cultural value this represents a practical and compassionate solution that brings a level of comfort previously available only in hospital settings.
At IBAP Clinics, we work with families to establish home-based PCA systems for appropriate patients, providing the training, equipment setup, and clinical support needed to manage complex cancer pain at home — where most Indian patients and families would choose to be.
For cancer pain localised to a specific limb, region, or nerve territory rather than diffuse visceral or spinal pain continuous peripheral nerve block catheters offer a highly targeted, opioid-sparing approach that can be maintained for days to weeks.
Using ultrasound guidance, a fine catheter is placed adjacent to a specific peripheral nerve or nerve plexus such as the brachial plexus at the interscalene or axillary level for arm pain, the femoral or sciatic nerve for leg pain, or the paravertebral space for chest wall and rib pain. A continuous infusion of local anaesthetic (typically ropivacaine or bupivacaine) is then delivered through this catheter, blocking pain transmission from the targeted nerve territory continuously, with patient-controlled bolus capability for breakthrough episodes.
Continuous peripheral nerve catheters deliver targeted analgesia without systemic opioid burden. The patient remains alert, orientated, and free of sedation, constipation, and nausea. The catheter can be managed at home for suitable patients, with remote guidance from the IBAP team. This is particularly valuable for patients who need to be as cognitively present as possible for family conversations, for treatment decision-making, or simply for the daily moments that matter.
All continuous peripheral nerve catheters at IBAP Clinics are placed under real-time ultrasound guidance, ensuring precise catheter tip placement adjacent to the target nerve, maximising analgesic efficacy, and minimising the risk of complications such as vascular puncture or nerve injury.
At IBAP Clinics Indo British Advanced Pain Clinics our approach to cancer pain management is built on a single, non-negotiable conviction: every patient deserves to live well, and every patient deserves to fight their cancer from a position of comfort rather than agony.
Dr Vijay Bhaskar Bandikatla trained and practised in the United Kingdom’s National Health Service before returning to Hyderabad to bring the same standard of specialist pain medicine available in London or Cambridge to patients in Telangana and Andhra Pradesh. This is not hyperbole the same image-guided techniques, the same evidence-based protocols, the same pharmacological expertise now available at Banjara Hills and Madeenaguda.
If you or a loved one is suffering from cancer pain that is not adequately controlled — whether newly diagnosed or having tried multiple medications — please contact us. A single consultation can often transform the trajectory of a patient’s comfort and quality of life. Call: 9807 55 6789 | Email: ibapclinics@gmail.com
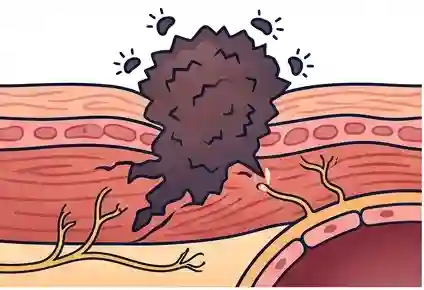
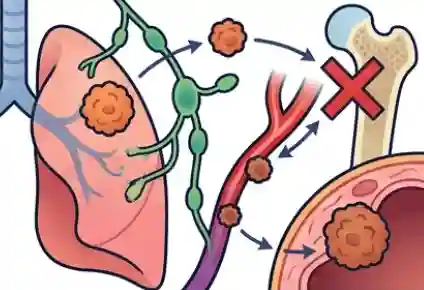
Cancer pain arises from multiple simultaneous mechanisms: direct tumour compression of nerves and organs; tissue erosion by infiltrating cancer cells; spread to distant organs (bone, liver, lung metastases); damage from chemotherapy (peripheral neuropathy); radiation-induced tissue injury and fibrosis; and pain from surgical removal of infiltrated structures. The severity arises because multiple pain types nociceptive, inflammatory, and neuropathic fire simultaneously, overwhelming simple analgesic approaches.
India consumes less than 1% of the world’s medical morphine despite bearing nearly 8% of global cancer deaths. The reasons are multiple: cultural fear of opioids and belief that morphine signals “the end”; regulatory barriers to prescribing; patients bypassing pain specialists and remaining under oncology follow-up alone; lack of specialist pain services outside major cities; and insufficient awareness both among patients and healthcare providers that effective interventional alternatives exist. IBAP Clinics exists to change this for patients in Hyderabad and beyond.
A neurolytic coeliac plexus block injects absolute alcohol or phenol around the coeliac plexus the nerve network near the aorta that relays upper abdominal pain under fluoroscopic or CT guidance. It provides significant pain relief in 70–90% of patients with pancreatic cancer, gastric cancer, liver metastases, and cholangiocarcinoma. Most patients experience relief within 24–48 hours, dramatically reducing opioid requirements, often allowing patients who had stopped eating to resume nutrition and re-engage with their oncological treatment.
Both systems deliver analgesic medications close to the spinal cord via a catheter, bypassing the systemic circulation and dramatically reducing required drug doses. The epidural catheter sits outside the dural sac, delivering local anaesthetic and opioid into the epidural space excellent coverage for thoracic, abdominal, and pelvic pain. The intrathecal catheter penetrates into the CSF surrounding the cord itself, delivering drugs at approximately 300× greater potency than the oral route. Both can be connected to external infusion pumps for home use a practical and cost-accessible approach that IBAP Clinics specialises in for Indian patients for whom a surgically implanted pump is not feasible.
Yes — and this coordinated approach is increasingly the gold standard. Radiotherapy is typically delivered first to shrink the tumour and devitalise cancer cells within the vertebra. Once RT is complete and the response is confirmed, kyphoplasty provides cement augmentation into the treated vertebral body, securing the bone against collapse and providing immediate, dramatic pain relief. This sequence provides both anti-tumour and mechanical pain benefits. In cases of impending fracture, the sequence may be adjusted a decision made jointly between the interventional pain specialist and radiation oncologist. At IBAP Clinics, we coordinate this directly with oncology colleagues.
Profoundly. Patients in severe uncontrolled pain frequently decline further chemotherapy, miss radiotherapy appointments, or refuse surgery not because the cancer has beaten them, but because the pain has. Families watching a loved one suffer daily begin to question whether continued treatment is kind, sometimes becoming advocates for stopping treatment. Depression almost universal in poorly controlled cancer pain chemically suppresses motivation and the capacity to imagine a better future. At IBAP Clinics, we have seen patients who had “given up” resume treatment and re-engage with life following successful pain intervention. Pain management is what makes cancer treatment possible.
Ketamine is available and used in India at IBAP Clinics as a supervised intravenous infusion for opioid-refractory cancer pain and opioid-induced hyperalgesia often with remarkable results for patients who have not responded to standard analgesics. Cannabis-based medicines are available in some forms in India; the regulatory landscape is evolving. At IBAP Clinics, we discuss all available and emerging therapeutic options transparently, including realistic assessment of access, cost, and expected benefit for each individual patient.


MBBS, DA, FRCA (UK), FFPMRCA (Pain Medicine, RCOA, UK)
CCT (Anesthesiology And Pain Management)
Neuromodulation & Advanced Pain Research Fellowship (London), MBA (HM)
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us