Helpline :
9807 55 6789
- Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
Your joint capsule has shrunk and tightened but a structured five-phase protocol restores full movement without surgery in most patients.

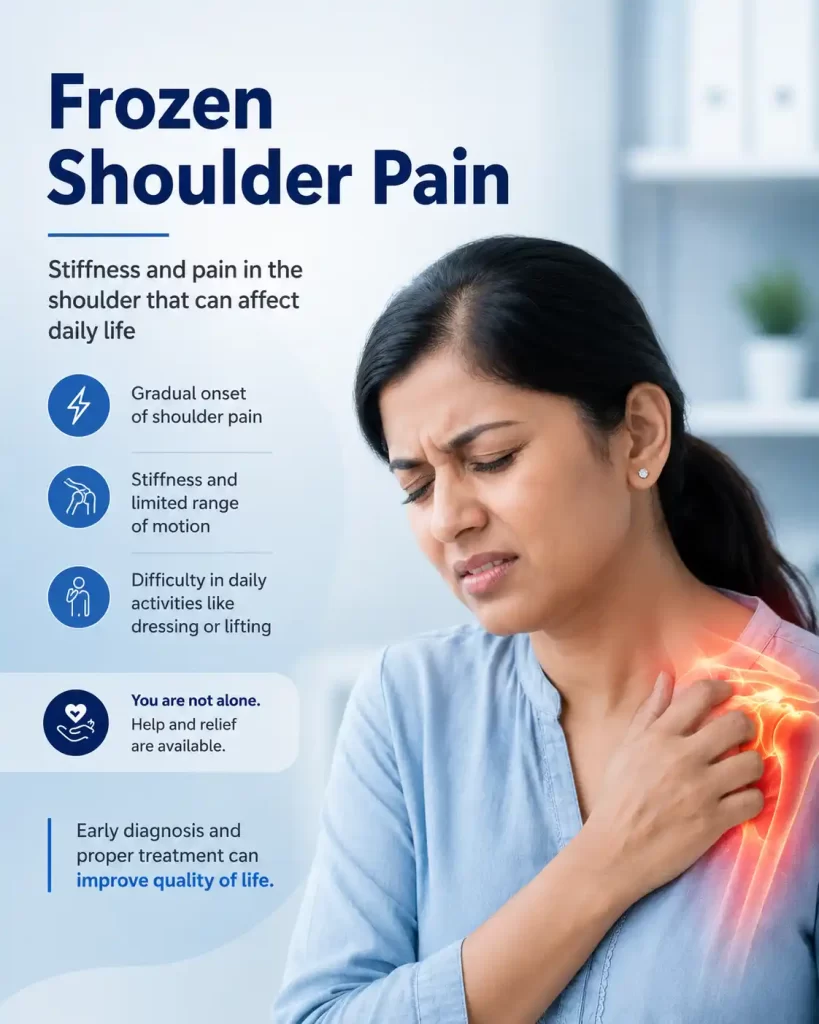
Frozen shoulder is a condition in which the lining around your shoulder joint called the joint capsule becomes inflamed, then gradually shrinks and forms thick bands of scar tissue. The result is a shoulder that is both painful and severely stiff.
The medical name, adhesive capsulitis, tells the story precisely: “adhesive” means the capsule sticks to itself with scar bands, and “capsulitis” means inflammation of the capsule. It affects roughly 2–5% of the general population and up to 20% of people with diabetes.
Crucially, frozen shoulder is not a rotator cuff tear, not arthritis, and not impingement. It is a disease of the capsule itself which is why treatment is quite different from other shoulder conditions.
Frozen shoulder follows a predictable but slow natural history.
Understanding which stage you are in guides the right treatment at the right time.

The most painful phase. Gradual aching pain worse at night and with movement. The shoulder is not yet severely stiff but is becoming so. Active inflammation is present inside the capsule.

Pain eases slightly, but stiffness dominates. Lifting the arm above shoulder height and external rotation become severely restricted. Scar tissue has thickened the capsule, reducing joint volume by up to 30%.

Movement slowly returns as the capsule reabsorbs scar tissue. Without intervention, this stage often leaves some residual muscle stiffness and weakness (atrophy). With the 5-phase protocol, recovery is compressed from years to weeks.
⚠️ Waiting for frozen shoulder to resolve on its own can take 2–3 years and often
leaves permanent joint stiffness and muscle weakness. A structured intervention at the right stage dramatically shortens this journey.

4–5× higher risk; more severe course; bilateral involvement common.
Hypo- and hyperthyroidism alter connective tissue, promoting fibrosis.

Perimenopausal hormonal changes affect connective tissue metabolism.

Immobilisation after injury or repair triggers secondary adhesive capsulitis.
Shared inflammatory pathways increase capsular fibrosis risk.
Reduced arm movement allows the capsule to contract progressively.
The diagnosis is primarily clinical based on your history and the pattern of movement restriction. However, imaging is essential to confirm the diagnosis, rule out other structural causes, and plan treatment.
Clinical Assessment
Dr Vijay uses a systematic examination assessing active and passive range of movement in all directions. In true adhesive capsulitis, both active and passive movement are equally restricted in a characteristic “capsular pattern” external rotation most limited, then abduction, then internal rotation.
MRI — The Essential First Step
MRI is performed to exclude full-thickness rotator cuff tears, labral pathology, significant degenerative change, or other structural causes of stiffness. It may also demonstrate capsular thickening and reduced capsular volume. Patients without full-thickness rotator cuff tears achieve bigger gains from hydrodilatation, supporting routine MRI in this context.
The variability in outcomes from single-step shoulder-joint steroid injections motivated a structured, phased approach — one that addresses each barrier to recovery in the correct sequence.
🔍Think of this like defrosting a frozen pipe: first you warm it gently (nerve block), then you flush it through under pressure (hydrodilatation), then you physically work the joint free (MUA), then you keep it moving with exercises (physio), then you continue to strengthen the joint with regular exercise. Each step prepares the shoulder for the next.
Under ultrasound guidance, a shoulder nerve block is performed a targeted injection around the shoulder nerves to fully numb the arm and eliminate muscle guarding. This step is essential: muscle spasm and pain guarding prevent effective distension or manipulation. The nerve block removes this resistance entirely.
Analogy: You would not try to iron a shirt while someone is pulling it tight. The nerve block lets the fabric relax first.
With the shoulder fully anaesthetised, a fine needle is guided precisely into the glenohumeral joint space using real-time imaging (ultrasound or fluoroscopy).
A carefully measured mixture is injected: typically 15–40 mL of sterile saline combined with a corticosteroid and local anaesthetic. The high volume physically stretches the shrunken capsule from the inside, breaking the adhesions causing restriction. The capsule may audibly “give” as the volume is infused.
The corticosteroid simultaneously dampens active inflammation. Patients without full-thickness rotator cuff tears achieve the greatest gains.
What you will feel: a sense of fullness or pressure during injection, followed by gradual relief over 24–72 hours. Some initial soreness is normal and settles quickly.
Immediately after hydrodilatation while the nerve block is fully active Dr.Vijay performs a controlled manipulation under anaesthesia (MUA).
With the shoulder completely pain-free, the arm is moved through its full range of motion in sequence: forward flexion, abduction, external rotation, and internal rotation. The goal is to physically break the remaining scar bands that the hydrodilatation volume alone could not fully release.
MUA performed in this sequence meets far less resistance and achieves greater range of motion gains.

Physiotherapy begins within 24 hours while the nerve block provides residual comfort.
Weeks 1–4 (ROM phase): pendulum swings, wall walks, pulleys, and assisted stretches. These maintain the capsular space created by the procedure.
Weeks 4–12 (progression phase): rotator cuff and scapular stabiliser exercises rebuild muscular control lost during months of disuse. Home exercise compliance is the single most important determinant of long-term outcome.
Patients who complete the physiotherapy programme achieve >80% return to full function at 12 weeks.

Routine physical exercises to maintain and further strengthen the shoulder muscles prevent recurrence and restore full functional capacity. This phase addresses the muscle atrophy that accumulates over months of restricted movement.
Scapular Rehab is a cornerstone of this phase: the scapular stabilisers (serratus anterior, lower and middle trapezius) are specifically targeted to restore normal scapulohumeral rhythm the coordinated movement between the shoulder blade and the arm that is disrupted by prolonged stiffness.
This ongoing strengthening programme distinguishes a full recovery from a partial one, and is what prevents the shoulder from gradually re-stiffening over subsequent months.
😌
Relaxation
Nerve block removes pain & guarding
💧
Hydrodistension
Volume injection stretches capsule
🤲
Manipulation
MUA breaks residual adhesions
🏃
Mobilisation
Early physio maintains capsular space
Strengthening
Scapular rehab & muscle rebuilding
E-E-A-T Credentials: Experience · Expertise · Authoritativeness · Trustworthiness
🔍Think of this like defrosting a frozen pipe: first you warm it gently (nerve block), then you flush it through under pressure (hydrodilatation), then you physically work the joint free (MUA), then you keep it moving with exercises (physio), then you continue to strengthen the joint with regular exercise. Each step prepares the shoulder for the next.
Dr Vijay Bhaskar Bandikatla MBBS, DA, FRCA (London), FFPMRCA (Pain Medicine), MBA (Hosp. Mgmt.), CCT (UK), Advanced Pain Training (Cambridge), DDSMed (Chicago), Fellowship in Neuromodulation & Advanced Pain (London).
Founder & Interventional Pain Specialist, IBAP Clinics (Banjara Hills & Madeenaguda, Hyderabad). Sr. Consultant, Apollo Hospitals, Hyderabad. Subspecialty trained in shoulder interventions and advanced pain procedures.
Protocol grounded in peer-reviewed literature: PubMed-indexed RCTs on hydrodilatation (UK FROST trial, Lancet 2020), AAPM&R guidelines on MUA, and Cochrane evidence on physiotherapy after capsular distension.
This article is for educational purposes only. It does not constitute personal medical advice. All treatment decisions should be made in consultation with a qualified pain specialist after clinical assessment and appropriate imaging.
Start your journey with a virtual consultation to discuss symptoms from home.
We review your medical history and relevant reports for a clear understanding.
Our doctors conduct a thorough assessment through detailed discussions.
We confirm findings with state-of-the-art imaging like X-rays, CT scans, and MRIs.
Our team identifies the root cause and key trigger points for treatment.
We create a customized treatment plan, including necessary medications and procedures.
Our Pain Specialists support a complete recovery focused on total wellness.
We provide ongoing follow-ups tailored to each treatment plan, ensuring continuous care and long-term recovery support.
We relieve your pain, helping you be yourself again!
Without treatment, frozen shoulder can last 18 months to 3 years, with up to 40% of patients retaining long-term stiffness. With the structured 5-phase protocol, most patients at IBAP Clinics achieve significant improvement in pain and range of movement within 6–12 weeks — compressing what the body would take years to achieve.
Because Phase 1 involves a shoulder nerve block, the arm is fully numb before any distension begins. Most patients feel mild pressure or a sensation of fullness during injection, but no sharp pain. Some post-procedure ache for 1–3 days is normal and managed with simple painkillers. Most patients drive themselves home the following day.
The vast majority of frozen shoulders even severe cases respond well to the non-surgical 5-phase protocol. Surgery (arthroscopic capsular release) is reserved only for patients who have failed 12+ months of structured conservative and interventional care, or those with a specific structural reason preventing adequate response to hydrodilatation and MUA.
Yes, the 5-phase protocol is safe for diabetics. Corticosteroid doses are carefully calibrated to minimise glycaemic impact. Close blood sugar monitoring is advised for 3–5 days after the procedure. The functional benefit significantly outweighs the temporary blood sugar rise risk for most patients.
A standard injection places 2–3 mL of steroid into the joint to reduce inflammation. While helpful early in the freezing stage, it does not address the capsular contracture. Hydrodilatation uses 15–40 mL of saline plus steroid and local anaesthetic to mechanically stretch the shrunken capsule from within — providing both chemical and mechanical treatment simultaneously.

EXCELLENTTrustindex verifies that the original source of the review is Google. Good pain relief with treatmentPosted on GoogleTrustindex verifies that the original source of the review is Google. Best for pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. बहुत अच्छा लगा हमें ये ट्रिटमेंट करा के अच्छे डॉक्टर और अच्छे स्टाफ हैं और काम पैसे में अच्छा अच्छा ट्रिटमेंट होता हैPosted on GoogleTrustindex verifies that the original source of the review is Google. Very nice, good and helpful staf, overall good experiencePosted on GoogleTrustindex verifies that the original source of the review is Google. Very good doctors and good tritment Thank you doctorPosted on GoogleTrustindex verifies that the original source of the review is Google. One of the best clinic for the relief of back painPosted on GoogleTrustindex verifies that the original source of the review is Google. Very good treatment indo british clinic for every pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. I have visited indo british pain clinic this is superb clinic for pain relief that's why I have given 5 start rating to this clinic ...Posted on GoogleTrustindex verifies that the original source of the review is Google. My name is Raja Sekhar Reddy Tummuri from kakinada city My father was suffering nervous pain from last 3 years … I have decided to join with this op … Now everything fine after treatment done from DR. vijay sir … Wonderful service received from INDO British advanced pain clinic Hospitals in Hyderabad @ Banjara Hills road no 12.. Each and every staff response , concern , support & everything it’s too good Thank you so much … Special thanks to Mr. DR. Vijay bhaskar Bandi Katla …👏🏻👏🏻👏🏻👏🏻🙏🙏Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
This article is written for educational and informational purposes. It does not replace a clinical assessment, diagnosis, or personalised treatment plan from a qualified medical professional. If you are experiencing shoulder pain, please consult a specialist. IBAP Clinics — Vijay Advanced Pain Clinics Pvt. Ltd., Hyderabad. ibapclinics@gmail.com · +91 98075 56789 · ibapclinics.com

MBBS, DA, FRCA (UK), FFPMRCA (Pain Medicine, RCOA, UK)
CCT (Anesthesiology And Pain Management)
Neuromodulation & Advanced Pain Research Fellowship (London), MBA (HM)
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us