Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
Let me be direct with you. Headaches and facial pain are not trivial. They are not "just stress." They are not something you should simply push through with a Crocin and a glass of water — though I understand entirely why so many people do exactly that. When you are rushing from Madhapur to Banjara Hills through peak-hour traffic, hitting every pothole on the route, your neck muscles braced against each jolt, your jaw clenched because the deadline at 5 pm is not going to move — you are building the perfect physiological storm for a head or facial pain episode.
India's lifetime prevalence of headache disorders exceeds 90 percent. The International Headache Society classifies over 150 distinct headache types across 14 categories. That is not a trivial number. It means that what you or your family member is experiencing is almost certainly a specific, diagnosable, and treatable condition. Not just "a headache."
In my years of practice — training first in the United Kingdom, then building IBAP Clinics here in Hyderabad — I have seen every type of head and facial pain imaginable. The retired school principal in her 60s who has had three-sided facial pain for years, told repeatedly it was dental. The 24-year-old software engineer working from home in Madhapur whose daily screen-time runs to 12 hours and whose occipital muscles feel like knotted rope. The teenage girl preparing for JEE in Secunderabad, getting attacks of visual aura before a pulsing headache every time her anxiety peaks around mock-test results. The homemaker from Madeenaguda who finds her worst migraine days are Tuesdays — the day she cooks lunch for 15 people before the afternoon temple visit.
All of these are real people. All of their pain is real. And all of them deserved better than being told to "rest and take it easy."
The single biggest clinical error I see — in emergency departments, in GP practices, even in some specialist settings — is treating all head pain as a single undifferentiated entity. It is a bit like going to a mechanic and being told "your car is making a noise" without them specifying whether it is the engine, the brakes, or a loose exhaust. The treatment is completely different depending on what is causing it.
Broadly, I think of head and facial pain in four major phenotypic groups. Neuropathic pain — where the nerve itself is injured or irritated, producing burning, shooting or electric sensations. Musculoskeletal pain — from the muscles of mastication, the cervical spine, the TMJ, or myofascial trigger points throughout the head and neck. Neurovascular pain — migraines and trigeminal autonomic cephalalgias, where a complex interplay of brain chemistry, blood vessel reactivity and neural sensitisation produces episodic, often severe attacks. And idiopathic pain — the "we have excluded everything else" category, which should only be assigned after a thorough and honest work-up.
The Trigemino-Cervical Complex (TCC) is a critical anatomical concept. It extends from the brainstem down to the C1–C2 spinal segments and explains why so many of our patients have both headache and neck pain simultaneously. The potholes of Hyderabad roads — jarring the cervical spine — are not just metaphorically giving you a headache. They physiologically can. Cervical input through the TCC directly amplifies trigeminal nociception.
Migraine is not just a bad headache. Let me say that again because it gets dismissed so often. Migraine is a neurological disorder with multiple recognised subtypes — migraine without aura, migraine with aura, hemiplegic migraine, vestibular migraine, retinal migraine, chronic migraine (≥15 days per month), menstrual migraine, and more. Many of my patients have come to me having suffered for years with what was told to them was "a sinus headache" — when in fact they had classic migraine. The sinus overlay in India is very common, and the confusion between the two is understandable but costly in terms of years of incorrect treatment.
A typical migraine attack causes intense, throbbing pain — usually one-sided — often accompanied by nausea, sensitivity to light, sensitivity to sound, and sometimes visual auras or neurological symptoms that precede the pain. Attacks last four hours to four days. They interfere completely with daily activities. And yet I have patients, particularly in the IT sector, who have been going to work through migraines for years, medicating with over-the-counter analgesics, unknowingly creating medication-overuse headache on top of the underlying migraine — a vicious cycle.
Think of the migraine brain as a smoke alarm with an unusually sensitive trigger. Normal smoke — a piece of burnt toast — should not set it off. But in a migraine-susceptible brain, the threshold is so low that even slight changes in sleep, stress hormones, bright light, or missing a meal can trip the alarm. The alarm itself (the headache) is real and severe. But the problem is the threshold setting, not just the immediate trigger. Our job is to reset the threshold — not just to silence the alarm each time it fires.
What triggers migraines in my Hyderabad patient population? Almost everything that defines modern urban Indian life. Skipping meals during fasting days or because work does not allow a lunch break. The strobe-like effect of fluorescent office lighting. The blue-light exposure from six to eight hours of computer and phone screens daily. Sleep deprivation before exams or quarterly appraisal season. The emotional tension of parents watching NEET or JEE rank lists. The physical tension of a long commute in stop-start traffic, neck muscles braced, jaw subtly clenched. A weekend at a loud film — even an enjoyable one — can tip a migraine-susceptible person over the edge.
Teenagers in particular are now presenting to my clinic with migraine at a rate that would have been unthinkable a decade ago. The pressure to perform — academically, socially, digitally — is genuinely physiological in its effects on the brain. I do not dismiss these as anxiety. I treat them as the neurological disorder they are, and I tell every young patient the same thing: your pain is not in your imagination, and you are not "too young" to have migraine.
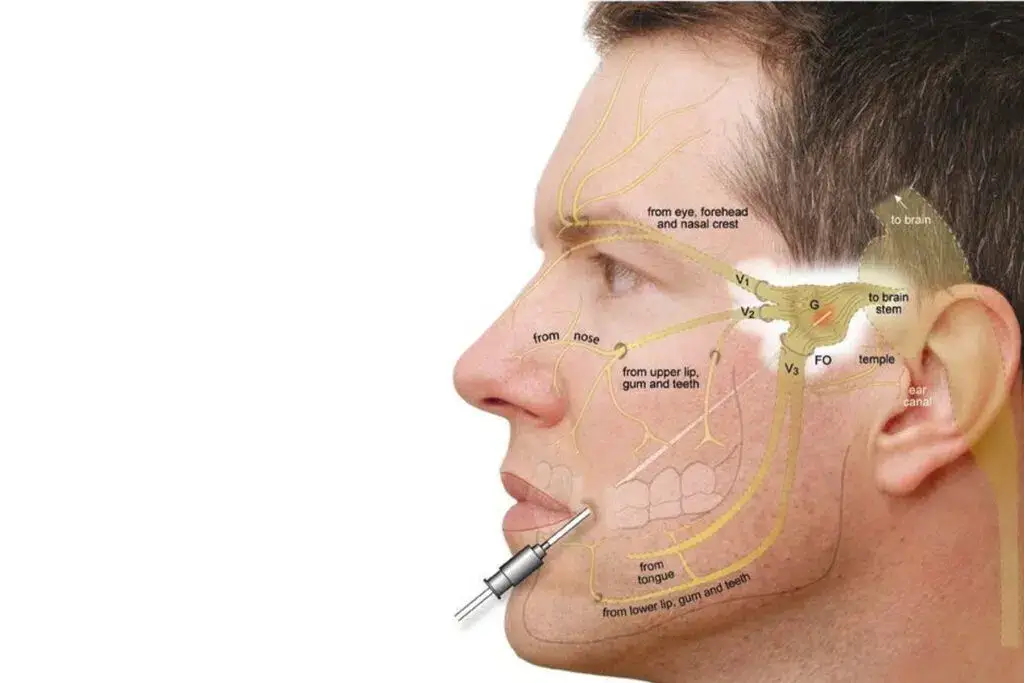
Facial pain is one of the most diagnostically challenging areas in all of pain medicine. The trigeminal nerve — which supplies sensation to virtually the entire face — has three major divisions: the ophthalmic (V1), maxillary (V2), and mandibular (V3). Pain anywhere in these distributions can mimic dental pain, sinus disease, or even cardiac pain. I have seen patients who have had multiple unnecessary dental extractions before the correct diagnosis of trigeminal neuralgia was made.
Classical trigeminal neuralgia is distinctive: brief, electric shock-like attacks, often triggered by chewing, talking, or light touch to the face. The pain is so severe that patients sometimes describe it as the worst thing they have ever experienced. Between attacks they may be entirely pain-free. The challenge is distinguishing this from secondary trigeminal neuralgia — caused by multiple sclerosis, tumour, or structural lesion — which requires high-resolution MRI of the trigeminal nerve pathways.
Trigeminal autonomic cephalalgias — cluster headache, paroxysmal hemicrania, SUNCT — are another group that far too often ends up in dentistry or ENT before reaching a pain specialist. Cluster headache produces excruciating unilateral orbital pain with ipsilateral autonomic symptoms: a watering eye, a drooping eyelid, a runny nostril. The autonomic involvement is the distinguishing feature and the clue to the therapeutic target — the sphenopalatine ganglion, which I discuss in detail below.
Myofascial pain from the temporomandibular joint and surrounding masticatory muscles is extraordinarily common, particularly in people who brux (grind their teeth) — which happens mostly during sleep and is strongly correlated with stress. The IT professional who works until midnight, stress-testing a product before launch, is grinding their teeth in their sleep. The student who lies in an awkward posture watching YouTube until 1 am is loading their cervical muscles in ways that translate directly into the next morning's headache.

Here is something I genuinely believe: the non-invasive treatment options for head and facial pain are woefully underutilised in India. People think neuromodulation means surgery. It does not. Some of the most effective neuromodulation technologies are completely external — you can wear them on your forehead, clip them to your ear, or have a session with a therapy device in a clinic without a single needle or incision.
TENS works by delivering small electrical pulses through skin-surface electrodes, activating large-diameter sensory nerve fibres that effectively "gate" incoming pain signals — much like how rubbing your elbow instinctively after knocking it provides relief. For cervicogenic headaches and tension-type headaches, TENS applied to the neck, suboccipital muscles, or pericranial region can meaningfully reduce pain intensity and frequency. Devices are relatively affordable and available for home use. It is not magic — but it is safe, evidence-backed, and often helpful as part of a broader programme. I frequently recommend it as an adjunct for patients who are managing chronic tension-type headache alongside pharmacotherapy.
Pulsed radiofrequency in its standard form is a minimally invasive technique — but external or transcutaneous pulsed RF is a truly non-invasive alternative. By delivering brief, pulsed electromagnetic fields to peripheral nerve regions, ePRF is thought to modulate nociceptive signalling at a cellular level without producing heat-based tissue damage. Evidence is still building, but there is meaningful published data on its use for trigeminal nerve distribution pain, occipital neuralgia, and myofascial pain states. In my practice I have seen patients benefit from this, particularly those for whom even a minor procedure is psychologically or medically contraindicated.
HILT — not to be confused with older low-level laser therapy — uses higher energy infrared laser pulses that penetrate more deeply into soft tissue, providing photobiomodulation effects at the level of muscle, tendon, fascia, and peripheral nerve. For patients with myofascial facial pain, TMJ-related head pain, or cervicogenic headache with pronounced muscular involvement, HILT can reduce inflammation, improve blood flow, and promote tissue healing. Clinic-based sessions over a few weeks are the usual approach. In India, high-quality HILT devices are now available at well-equipped pain and physiotherapy centres.
Cefaly is, in my view, one of the most clinically impressive non-invasive devices available for migraine. It is a small, headband-worn device that positions an electrode on the forehead and delivers precise electrical stimulation to the supratrochlear and supraorbital branches of the trigeminal nerve — desensitising the trigeminal pathway over time. The TEAM (Trial of External Trigeminal Nerve Stimulation for the Acute Treatment of Migraine) study showed 79 percent of users achieved pain relief following one hour of acute treatment, with 32 percent achieving complete pain freedom. The 20-minute daily prevention programme reduces attack frequency with regular use.
The Cefaly device is FDA-cleared and available in India. I strongly recommend it to patients who are intolerant of migraine medications, who are pregnant, or who want a drug-free option they can use at home. I have personally seen a middle-aged woman from Madeenaguda — a homemaker who could not tolerate triptans due to cardiovascular concerns — achieve remarkable improvement in her chronic migraine with consistent Cefaly use alongside lifestyle adjustment.
The gammaCore device delivers non-invasive electrical stimulation to the vagus nerve at the neck. It is FDA-approved for both acute and preventive treatment of episodic and chronic cluster headache, and for acute migraine treatment. The vagal pathway influences GABAergic and serotonergic signalling and modulates descending pain inhibition through the trigemino-cervical complex. For cluster headache in particular — which is arguably the most painful condition in clinical medicine — nVNS provides a meaningful non-invasive option between attacks and can abort individual episodes.
rTMS uses rapidly changing magnetic fields to induce electrical currents in cortical neurons — without any surgical access whatsoever. A coil is placed against the scalp and brief magnetic pulses target specific brain regions. For migraine prevention, rTMS targeting the motor cortex or dorsolateral prefrontal cortex has shown meaningful reductions in headache frequency in randomised trials. For depression comorbid with chronic pain — which is genuinely very common — rTMS has an established therapeutic role. Single-pulse TMS (sTMS) is also approved for acute migraine treatment. In India, rTMS is increasingly available in metropolitan centres and is worth considering for patients with high-frequency migraine who have not responded adequately to medications or who have significant mood comorbidity.
| Device / Technique | Target | Best Indication | Evidence Level | Home Use? |
|---|---|---|---|---|
| TENS | Peripheral sensory fibres (gate control) | Tension-type headache, cervicogenic headache | Moderate (Class II-III) | Yes |
| External PRF (ePRF) | Peripheral nerve — pulsed EM modulation | Occipital neuralgia, trigeminal distribution pain | Limited (observational series) | Clinic-based |
| HILT | Muscle, fascia, peripheral nerve (photobiomodulation) | Myofascial facial/head pain, cervicogenic headache | Moderate (growing RCT data) | Clinic-based |
| Cefaly (eTNS) | Supraorbital / supratrochlear branches V1 | Migraine — acute & prevention | Strong (RCT; FDA-cleared) | Yes |
| nVNS (gammaCore) | Vagus nerve at neck | Cluster headache (acute + prevention), migraine acute | Strong (RCT; FDA-approved) | Yes |
| rTMS | Motor cortex / DLPFC | Migraine prevention, comorbid depression | Strong (multiple RCTs) | Clinic-based |
| sTMS (single-pulse) | Occipital cortex | Acute migraine with aura | Moderate (FDA-cleared) | Yes (device rental) |
The sphenopalatine ganglion (SPG) is a small collection of nerve cells sitting behind the nasal cavity, just lateral to the sphenoid bone. It is a key relay station for cranial autonomic outflow — the pathway that produces the watering eye, runny nostril, and facial flushing seen in cluster headache and some migraines. It also has connections to the trigeminal nerve, making it relevant to a broader range of facial pain syndromes.
The sphenopalatine ganglion is like the central junction box of a building's wiring system — sitting hidden behind the walls, routing signals between the autonomic and sensory systems. Blocking it is like throwing the correct circuit breaker: the lights in that entire circuit go out, interrupting the pain signal cascade at its origin.
An SPG block can be performed in several ways. The simplest is the intranasal cotton-tip method — a long cotton-tipped applicator soaked in local anaesthetic is passed gently along the nasal passage to rest adjacent to the ganglion. The patient lies still for 20–30 minutes. It sounds simple because it is — but the effects can be dramatic. For an acute migraine or cluster headache attack, relief can begin within minutes. For chronic migraine prevention, a series of SPG blocks over several weeks can meaningfully reduce attack frequency.
More precise delivery uses a purpose-built intranasal catheter device (such as the SphenoCath or Tx360) which allows a small amount of local anaesthetic to be expressed directly against the ganglion mucosa. In selected refractory cases — particularly chronic cluster headache — a minimally invasive fluoroscopy- or CT-guided injection to the SPG delivers a depot of local anaesthetic or corticosteroid with high precision.
For truly refractory chronic cluster headache that has failed all medical and simpler interventional options, implantable SPG stimulation devices are now available. The pivotal sham-controlled trial showed pain relief in 62.46 percent of stimulation-treated attacks versus 38.87 percent in the control condition. Long-term data show efficacy persisting beyond one year. This is genuinely transformative for patients whose cluster headache has made their lives barely liveable.
Peripheral nerve blocks involve injecting a small volume of local anaesthetic — sometimes with or without steroid — adjacent to specific nerves. They serve dual purposes: diagnostic (confirming the pain generator) and therapeutic (providing lasting relief beyond the local anaesthetic duration, possibly through modulation of central sensitisation).
The greater occipital nerve block is the most commonly performed and most evidence-backed. It targets the greater occipital nerve at the back of the skull and is used for occipital neuralgia, cervicogenic headache, chronic migraine, and cluster headache. Relief often extends well beyond what a simple anaesthetic would predict — sometimes weeks to months — suggesting genuine neuromodulatory effects on the trigemino-cervical complex.
Other relevant peripheral blocks for head and facial pain include the supraorbital and supratrochlear nerve blocks (for frontal headache and V1 distribution pain), infraorbital nerve block (for V2 distribution facial pain), auriculotemporal nerve block (for temporomandibular and temporal pain), and mental nerve block (for lower facial and chin pain). In skilled hands, these are safe, quick, and often profoundly effective.
| Intervention | Invasiveness | Best For | Duration of Effect | Available at IBAP? |
|---|---|---|---|---|
| Greater Occipital Nerve Block | Minimally invasive | Cervicogenic H/A, chronic migraine, cluster | Weeks to months | Yes |
| SPG Block (intranasal) | Non/minimally invasive | Acute migraine, cluster headache | Hours to weeks | Yes |
| Botox (Chronic Migraine) | Minimally invasive | Chronic migraine (≥15 days/month) | ~12 weeks per cycle | Yes |
| Botox (Trigeminal Neuralgia) | Minimally invasive | Refractory TN, myofascial jaw pain | ~12–16 weeks | Yes |
| Radiofrequency Ablation (Gasserian) | Minimally invasive — fluoroscopy guided | Classical TN — V2/V3 | 1–3 years | Yes |
| Peripheral Nerve Stimulation (implant) | Minimally invasive surgery | Supraorbital, infraorbital, occipital neuropathy | Long-term (adjustable) | Yes |
| Occipital Nerve Stimulation (implant) | Minimally invasive surgery | Refractory chronic migraine, occipital neuralgia | Long-term (adjustable) | Yes |
| SPG Stimulator (implant) | Minimally invasive surgery | Refractory chronic cluster headache | Long-term (patient-controlled) | Yes — selected cases |
Let me address this directly because I hear the confusion so often. Botulinum toxin type A (onabotulinumtoxinA) is not primarily a cosmetic product — it is a powerful neurological agent that happens to also have cosmetic applications. In the pain world, Botox is FDA-approved for chronic migraine and has compelling evidence in trigeminal neuralgia, myofascial orofacial pain, and bruxism-related jaw pain.
For chronic migraine, the PREEMPT protocol involves injections at 31 fixed sites across the head and neck — the corrugator, frontalis, occipitalis, cervical paraspinal muscles, and others — every 12 weeks. The mechanism goes beyond muscle relaxation: Botox inhibits peripheral release of nociceptive mediators including substance P, glutamate, and CGRP. This means it acts on the sensitised pain pathways themselves, not just the muscle tightness. A 2024 systematic review and meta-analysis of randomised and non-randomised studies showed approximately 71 percent of trigeminal neuralgia patients achieved at least 50 percent reduction in pain scores.
I have had patients — particularly older professionals and homemakers in their 40s and 50s who cannot tolerate the side effects of carbamazepine or who have not responded adequately to it — achieve genuinely life-changing improvement with a Botox programme for trigeminal neuralgia. The side effects are usually transient and local: mild swelling, occasional temporary facial asymmetry. It is not perfect. But for the right patient, it is remarkable.
I want to speak plainly about something that matters deeply to me. A very large proportion of patients who come to my clinic with head and facial pain have been dismissed somewhere along their journey. "It is just stress." "Everyone gets headaches." "You are anxious — try to relax." These phrases have been said by well-meaning doctors, by family members, sometimes even by specialists. And they are scientifically wrong.
Chronic pain — whether migraine, trigeminal neuralgia, persistent facial pain, or any other form — changes the nervous system. It causes measurable, demonstrable neuroplastic changes. The sensitisation is real. The suffering is real. And the functional disability — missing your child's school performance, being unable to drive because the road vibration triggers an attack, having to turn away from a film because the sound is unbearable — is real and significant.
Research has now demonstrated something that I believe intuitively and have seen clinically for years: the quality of the therapeutic relationship — whether the patient feels genuinely heard and validated — independently predicts pain outcomes. A 2022 paper in PAIN showed that higher physician empathy scores correlated with better functional outcomes at 6-month follow-up in chronic pain patients. This is not soft science. The experience of feeling understood changes how the nervous system processes pain signals.
My philosophy has not changed in 20 years of practice. Every patient who sits in front of me is having the worst version of their own experience. Not a worse experience than yours or mine — the worst version of their own. That frame of reference is everything. The homemaker who cannot get out of bed with a migraine on a Sunday when she is supposed to host the family is having a catastrophic day. The teenager who cannot sit her exam because of a trigeminal attack is having a catastrophic day. They do not need to be compared to someone else's pain. They need to be seen, believed, and helped.
You deserve a proper diagnosis and a treatment plan that goes beyond "take painkillers and rest." Contact IBAP Clinics to arrange a consultation with Dr Vijay Bhaskar Bandikatla at our Banjara Hills or Madeenaguda clinic.
2nd Floor, 284/A, Road No. 12
Above IDFC First Bank, near Omega Hospitals
MLA Colony, Banjara Hills
Hyderabad, Telangana 500034
Sy No. 2, 4th Floor, Plot No. 200
Beside South India Shopping Mall
Opp. Fortune Heights, Mythri Nagar
Madeenaguda, Hyderabad, Telangana 500049

