Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
From the Carnett sign and clinical taxonomy to coeliac plexus neurolysis, splanchnic RF ablation, TAP blocks, spinal cord stimulation, and the gut-brain axis — a complete guide by Dr Vijay Bhaskar Bandikatla, IBAP Clinics.

Many people in Hyderabad come to me and say exactly this: “Doctor, all my tests are normal, but my stomach pain is still there. Is it only in my mind?” And honestly I hear this every single week. From software engineers in Madhapur who sit ten hours at a desk. From teenagers in coaching centres in Ameerpet who skip breakfast and survive on tea and biscuits. From homemakers who have been managing three things at once for years. From elderly patients who drove forty minutes across Banjara Hills on potholed roads arriving with pain that nobody has been able to explain.
The pain is not in your mind. And the dismissal “your reports are normal, you are fine” is one of the most damaging things a patient can hear. It does not erase the pain. It erases the person.
At IBAP Clinics, my approach is clear. First believe your pain. Second understand where it is actually coming from. Third use targeted, safe, interventional techniques to address that source directly when routine medications have run out of answers.
Think of it like this. If your abdominal pain has become an unwanted tenant in your house, I am not handing you earplugs in the form of painkillers. I want to find exactly where that tenant is hiding organ, nerve, muscle wall, or brain-gut axis and, scientifically and gently, ask him to leave. Each hiding place needs a completely different eviction notice.
Chronic abdominal pain lasting more than three to six months that has failed to respond to standard treatment is not a dead end. It is the beginning of a more precise diagnostic process. The key question is always: visceral organ? Abdominal wall? Functional gut-brain axis? Neuropathic nerve injury? The answer determines everything that follows.
chronic abdominal pain originates from the abdominal wall frequently missed
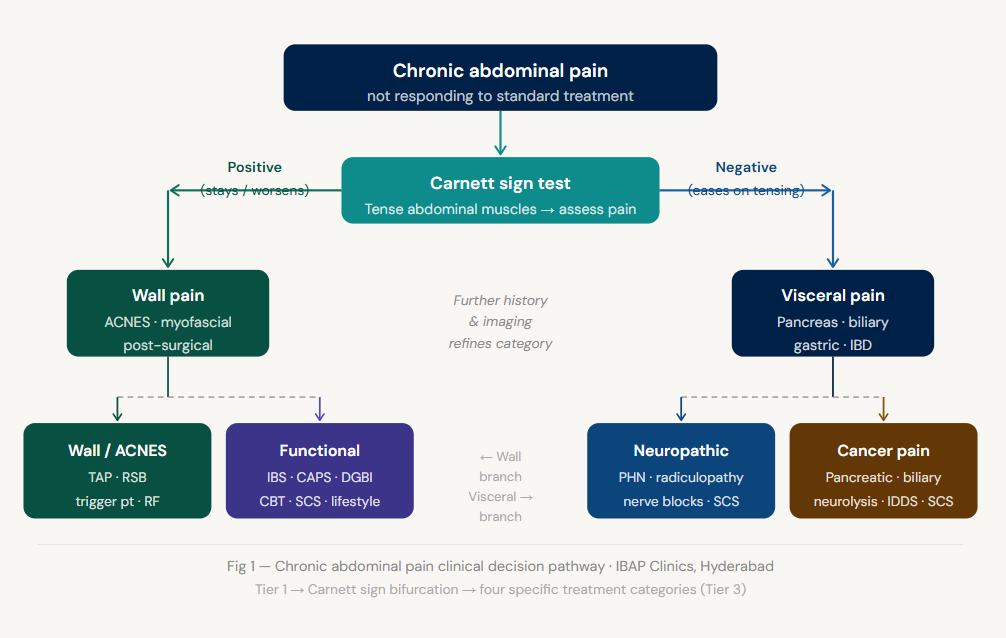
Before any treatment can be planned, the pain must be classified. This is the foundation of the interventional pain approach and the step most often skipped in general medical settings. There are four distinct categories, and they require entirely different treatments.
This is pain arising from internal organs the pancreas, stomach, liver, biliary system, intestines, or malignancy. The character is typically deep, dull, and cramping; poorly localised; often referred to the back; worsened or triggered by food. It may come with nausea, vomiting, weight loss, or change in bowel habit. The pain signals travel through the splanchnic nerves and the coeliac plexus which makes these nerve networks the primary interventional targets.
This is perhaps the most frequently missed diagnosis in all of abdominal pain medicine. Anterior Cutaneous Nerve Entrapment Syndrome ACNES occurs when the small sensory branches of the thoracic intercostal nerves become trapped as they pierce the rectus abdominis muscle. The pain is sharp, well-localised the patient can point with one finger worsened by movement and muscle tensing, and entirely unrelated to eating or bowel function.
This pain does not show up on a CT scan. It does not appear in blood tests. But it is real, it is common, and it responds beautifully to a simple injection. The diagnosis requires one bedside manoeuvre the Carnett sign.
When all scans, endoscopies, and blood tests come back entirely normal yet the pain is real, frequent, and ruining daily life we are often dealing with a disorder of gut-brain interaction (DGBI). The nervous system has become over-sensitised. Normal things digestion, mild gas, the usual stretching of the bowel after a meal suddenly feel like severe pain. The wiring is amplifying signals that should be silent.
In Hyderabad today, I see this pattern constantly. Teenagers under relentless exam pressure presenting with IBS-like abdominal pain. Software employees working twelve-hour days, eating at odd hours, ordering in at midnight. The gut-brain axis responds to stress like a loudspeaker with feedback it amplifies. It does not invent the sound. It just makes it unbearably loud.
Always screen patients who have been on chronic opioids for “undiagnosed” abdominal pain. Paradoxically, long-term opioid use can actually worsen abdominal pain through opioid-induced gut hypersensitivity. The patient and prescribing doctor both assume more opioid means less pain. In fact, the opioid is the cause. Recognition is critical treatment involves carefully tapering the opioid, the opposite of the usual instinct.
Sometimes the pain in the front of the abdomen is coming from the back. A thoracic disc prolapse, a compressed nerve root at T7 to T12, post-herpetic neuralgia after shingles all of these can cause burning, electric-shock sensations, or crawling paraesthesiae in the abdominal wall that are entirely unrelated to any abdominal organ. The source is the spine; the symptom is in the tummy. Patients describe it as “ants crawling under the skin” or “a hot wire.” Missing this leads to years of unnecessary gastroenterological investigation.
I do not think this is only about biology. What I see in Hyderabad clinics every week tells a social story as much as a medical one.
Teenagers are arriving with abdominal pain driven by the pressure of school ranks, board results, entrance exams. They eat irregularly skipping breakfast, surviving on biscuits and tea during coaching hours, then eating heavily at night. Sleep is disrupted by screens, anxiety, and social media comparison. The gut-brain axis in an adolescent is extraordinarily sensitive, and we are stressing it systematically.
Software employees sit for ten to twelve hours with multiple monitors, driven by deadlines and review cycles. They eat at odd times Swiggy at 11pm, coffee as breakfast. The spine takes a beating from poor chair ergonomics and no movement. Then the evening commute on Hyderabad roads potholes, speed breakers, aggressive lane changes jars the spine further. Poor sleeping posture at home completes the picture.
Middle-aged and elderly patients have a different pattern. Long drives to temples, movies, social gatherings wonderful activities, but often on bad roads, in poor posture, for long durations. The result: spinal nerve irritation that presents as abdominal pain, or genuine visceral pain that has been dismissed too long because “at your age, some pain is normal.” It is not normal. And it is not acceptable.
Homemakers are perhaps the most overlooked. Continuous multitasking, irregular meals, delayed medical attention because the family’s appointments always come first. I have seen women who have had abdominal pain for three years and never prioritised getting it assessed properly.
Pain is not only from organs. It is from lifestyle, stress, posture, sleep, irregular food, and very importantly from the absence of empathy. When a doctor or family member says “all your tests are normal, you are fine,” it does not reassure the patient. It erases them. And erased patients delay care, escalate anxiety, and ultimately present later with more complex problems.
First described by John Berton Carnett in 1926, this test has stood for a century. And yet I find it is almost never performed in general practice or gastroenterology settings. Patients arrive at my clinic having had three CT scans, an MRI, a colonoscopy, and a gastroscopy. Nobody has done Carnett’s test. It takes thirty seconds.
An additional clinical pearl: abdominal wall pain patients can usually point to their pain with one finger — a small, finger-tip-sized spot. Visceral pain patients sweep their hand across a wide area. That one observation, before you even do Carnett’s test, is already telling you where to look.
Before any pain clinic pathway is planned, red flags must be excluded. These features indicate a potentially serious underlying pathology requiring urgent specialist assessment, not just pain management.
At IBAP Clinics, if any red flag is present on assessment, we coordinate immediately with gastroenterology or surgery colleagues. Your safety always comes before any interventional procedure.
When you visit us, the first consultation takes thirty to forty-five minutes. This is not bureaucracy — it is the diagnostic work without which no safe intervention can be planned.

When did pain start, how does it feel cramping, burning, stabbing, dull. What triggers it: food, stress, movement, posture, long sitting, driving on bumpy roads. Relationship to motions, urination, menstrual cycle. Sleep pattern, occupation, and lifestyle.





Where needed, we align closely with the patient’s gastroenterologist to ensure no occult pathology SIBO, low-grade IBD, microbiome dysbiosis is missed before proceeding to interventional management.
Interventional pain management for chronic abdominal pain is precisely matched to the category of pain identified during assessment. What works beautifully for visceral pancreatic pain does nothing for abdominal wall nerve entrapment and vice versa.
When Carnett’s sign is positive when the pain is small, finger-pointable, worsened by movement, with normal imaging the abdominal wall is the target.
Local anaesthetic sometimes with steroid injected directly into the most painful spot. Often gives immediate relief within minutes. Confirms diagnosis if pain improves by more than 50%. Can be repeated for sustained benefit.
For deep visceral pain from chronic pancreatitis, malignancy, or severe gut pain, the target is the sympathetic nervous system specifically the plexuses and ganglia that relay pain signals from the internal organs.
For a carefully selected subgroup of patients with refractory visceral abdominal pain where organ-directed treatments, nerve blocks, and all medications have provided insufficient relief spinal cord stimulation offers a transformative option. A thin electrode is placed near the dorsal spinal cord through a needle, typically at the thoracic level. A small implanted device sends gentle, programmable electrical impulses that modify how pain signals are processed.
Think of it as a volume controller on the pain pathway. The underlying signal may still exist but the brain stops receiving it at the volume that was making life impossible. Multiple studies show improvement in pain scores, functional capacity, and reduction in opioid use for chronic visceral pain. And critically we always do a trial first. A temporary electrode for five to seven days. Only if the trial is successful do we plan permanent implantation.
In patients with severe cancer-related abdominal pain where oral opioids provide inadequate relief or cause intolerable side effects severe constipation, drowsiness, cognitive impairment intrathecal drug delivery is a highly effective option. A small programmable pump delivers tiny doses of opioid directly into the cerebrospinal fluid near the spinal cord. Because the drug is delivered so close to its site of action, the effective dose is typically one-three hundredth of the oral dose. Dramatically less side-effect burden. Dramatically better relief. Always planned in close collaboration with oncology and palliative care teams.
For functional abdominal pain, IBS, and disorders of gut-brain interaction, tablets and nerve blocks alone are not sufficient. Research is increasingly clear that combining medical treatment with psychological and lifestyle approaches gives substantially better long-term results. I always tell my patients: “Your pain is real. But your nervous system is trainable.”
| Procedure | Pain Category | Evidence | Duration of Benefit | Guidance Used |
|---|---|---|---|---|
| Trigger point injection | Abdominal wall (ACNES) | Good | Weeks–months | Ultrasound |
| TAP block | Abdominal wall | High (surgical) | 12–24 hrs single; extended with catheter | Ultrasound |
| Rectus sheath block | Midline wall pain | Moderate | 8–16 hrs | Ultrasound |
| Subcostal / OSTAP block | Upper abdominal wall | Moderate | 12–18 hrs | Ultrasound |
| ILIH nerve block / RF | Lower wall / post-hernia | Moderate | RF: 6–12 months | Ultrasound / Fluoroscopy |
| Coeliac plexus block | Visceral / pancreatitis | High (RCT) | 4–12 weeks | CT / Fluoroscopy / EUS |
| Coeliac plexus neurolysis | Pancreatic / biliary cancer | High (multiple RCTs) | Months–lifetime | CT / Fluoroscopy / EUS |
| Splanchnic nerve block | Upper visceral / pancreatitis | Moderate–High | 6–12 weeks | Fluoroscopy / CT |
| Splanchnic RF ablation | Pancreatic Ca / pancreatitis | Moderate (case series) | 6–12 months | Fluoroscopy |
| Superior hypogastric block | Lower visceral / pelvic cancer | Moderate | Weeks–months | Fluoroscopy / CT |
| Lumbar epidural infusion | Acute pancreatitis flare | Moderate | Days–weeks | Fluoroscopy |
| Spinal cord stimulation | Refractory visceral pain | Moderate–High | Ongoing (implant) | Fluoroscopy |
| Intrathecal pump (IDDS) | Advanced cancer pain | High | Ongoing (implant) | Fluoroscopy |
Bring all old reports scan CDs, discharge summaries, endoscopy reports, blood test results. Nothing will be discarded; everything tells us something. WhatsApp or email reports in advance if possible.
Understanding and empathy are not soft skills in pain medicine. They are active components of treatment. The science is unambiguous: a compassionate consultation improves pain outcomes, reduces anxiety, and enhances the response to interventional procedures. When I tell a patient “I believe you, and there are things we can do” — that is not just kindness. It is clinical practice. I have seen patients cry in the consultation room — not from pain, but from the relief of finally being believed. That moment matters. And it is the foundation of everything that follows.
Start your journey with a virtual consultation to discuss symptoms from home.
We review your medical history and relevant reports for a clear understanding.
Our doctors conduct a thorough assessment through detailed discussions.
We confirm findings with state-of-the-art imaging like X-rays, CT scans, and MRIs.
Our team identifies the root cause and key trigger points for treatment.
We create a customized treatment plan, including necessary medications and procedures.
Our Pain Specialists support a complete recovery focused on total wellness.
We provide ongoing follow-ups tailored to each treatment plan, ensuring continuous care and long-term recovery support.
We relieve your pain, helping you be yourself again!
Normal investigations do not mean no pain. Chronic abdominal pain can arise from the abdominal wall (nerve entrapment that does not show on imaging), the gut-brain axis (visceral hyperalgesia that does not show on endoscopy), neuropathic nerve injury from the thoracic spine, or deeper organ changes that standard imaging misses at early stages. An interventional pain assessment including the Carnett sign bedside test and targeted diagnostic nerve blocks can identify the true source and guide a precise treatment plan.
Anterior Cutaneous Nerve Entrapment Syndrome (ACNES) is a frequently missed condition where small sensory nerves become trapped as they pierce the rectus abdominis muscle. The pain is sharp, localised to a small area at the lateral rectus edge, finger-pointable, worsened by movement and muscle tensing, and positive on Carnett’s test. It is treated initially with a trigger point injection of local anaesthetic and steroid often giving dramatic immediate relief. For recurrent cases, radiofrequency ablation or pulsed RF of the identified cutaneous nerve provides months of benefit.
Narcotic bowel syndrome is a paradoxical condition where long-term opioid use actually worsens abdominal pain through opioid-induced gut hypersensitivity and central sensitisation. It is suspected when a patient on chronic opioids reports escalating abdominal pain despite increasing doses. Treatment involves carefully supervised opioid tapering which counterintuitively reduces pain as the opioid is withdrawn. This must be done under medical supervision with appropriate adjunctive support.
Yes, in most cases. Coeliac plexus block with local anaesthetic and steroid provides weeks to months of meaningful relief and can be repeated. Splanchnic nerve radiofrequency ablation gives six to twelve months of benefit and is repeatable. Lumbar epidural infusions are effective for acute-on-chronic flares. Surgery for ductal drainage or pancreatic resection is reserved for specific structural anatomical problems, not for pain management alone in most patients.
Seek urgent medical assessment if you have any of the following alongside your abdominal pain: unintentional weight loss, fever, blood in stool or vomiting of blood, jaundice (yellow eyes or skin), severe pain that wakes you from sleep at night, a palpable lump in the abdomen, or new onset of pain over the age of 50 with no prior history. These red flags require investigation by a gastroenterologist or surgeon before any pain management is planned.
Spinal cord stimulation involves placing a thin electrode near the dorsal spinal cord, connected to a small implanted device that delivers programmable electrical impulses. These impulses modify the way pain signals are processed acting like a volume controller on the pain pathway. The underlying source of pain may still exist, but the brain no longer receives it at the intensity that was disabling daily life. A mandatory trial period of five to seven days is always performed before any decision about permanent implantation.
An intrathecal drug delivery system (IDDS) delivers opioid medication directly into the cerebrospinal fluid surrounding the spinal cord. Because the drug reaches its site of action directly, the effective dose needed is typically one-three hundredth of the oral dose meaning dramatically less drowsiness, less constipation, less nausea, and better pain relief. It is considered for advanced cancer pain in patients where oral opioids have become either ineffective or intolerable.

EXCELLENTTrustindex verifies that the original source of the review is Google. Good pain relief with treatmentPosted on GoogleTrustindex verifies that the original source of the review is Google. Best for pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. बहुत अच्छा लगा हमें ये ट्रिटमेंट करा के अच्छे डॉक्टर और अच्छे स्टाफ हैं और काम पैसे में अच्छा अच्छा ट्रिटमेंट होता हैPosted on GoogleTrustindex verifies that the original source of the review is Google. Very nice, good and helpful staf, overall good experiencePosted on GoogleTrustindex verifies that the original source of the review is Google. Very good doctors and good tritment Thank you doctorPosted on GoogleTrustindex verifies that the original source of the review is Google. One of the best clinic for the relief of back painPosted on GoogleTrustindex verifies that the original source of the review is Google. Very good treatment indo british clinic for every pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. I have visited indo british pain clinic this is superb clinic for pain relief that's why I have given 5 start rating to this clinic ...Posted on GoogleTrustindex verifies that the original source of the review is Google. My name is Raja Sekhar Reddy Tummuri from kakinada city My father was suffering nervous pain from last 3 years … I have decided to join with this op … Now everything fine after treatment done from DR. vijay sir … Wonderful service received from INDO British advanced pain clinic Hospitals in Hyderabad @ Banjara Hills road no 12.. Each and every staff response , concern , support & everything it’s too good Thank you so much … Special thanks to Mr. DR. Vijay bhaskar Bandi Katla …👏🏻👏🏻👏🏻👏🏻🙏🙏Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more
This article is written for educational and informational purposes only and does not constitute medical advice, diagnosis, or a treatment plan for any individual patient. The clinical information reflects the professional experience and opinions of Dr Vijay Bhaskar Bandikatla and current published literature; individual patient circumstances vary significantly. Interventional pain procedures carry risks that must be discussed in detail during a formal consultation. If you are experiencing abdominal pain — particularly with any red flag symptoms — please seek assessment from a qualified medical professional without delay. IBAP Clinics, Hyderabad accepts no liability for decisions made solely on the basis of this article.

MBBS, DA, FRCA (UK), FFPMRCA (Pain Medicine, RCOA, UK)
CCT (Anesthesiology And Pain Management)
Neuromodulation & Advanced Pain Research Fellowship (London), MBA (HM)
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us