Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
There is a particular kind of exhaustion that comes with chronic pain. Not just the knee aching every time you climb the stairs, or the back seizing up the moment you sit at your desk. It is the exhaustion of being told — politely, repeatedly — that you must either learn to live with it, or eventually book yourself in for surgery. That you have, in effect, run out of options.
I hear this story constantly at IBAP Clinics. People arrive having done everything that was suggested — every exercise, every anti-inflammatory, every course of physiotherapy — and they are still in pain. So when I start explaining prolotherapy, there is often a flicker of scepticism. A sugar injection? For a torn ligament? For a knee that has been failing for two years? It sounds almost too simple to be taken seriously.
But the simplest solutions are sometimes the most effective. The science behind prolotherapy has been building quietly for decades in peer-reviewed journals, and for the right patient, the results are genuinely meaningful.
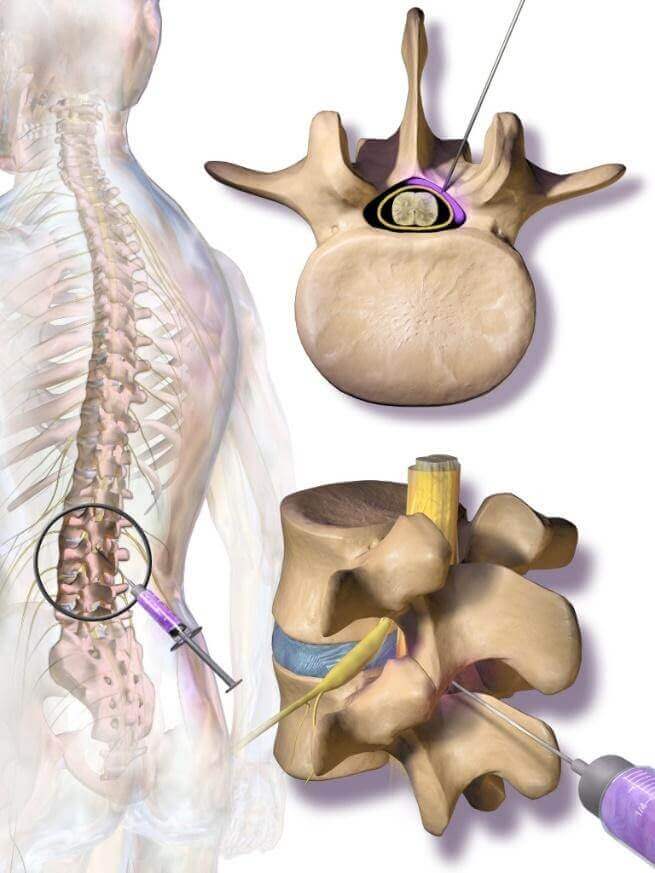
Prolotherapy — from proliferation therapy, meaning it stimulates new tissue growth — involves injecting a solution of concentrated dextrose (glucose sugar) precisely into or around damaged tissue: ligaments, tendons, joint spaces, muscle trigger points, or nerve sheaths. The dextrose concentration is chosen based on target tissue, ranging from 5% for nerves to 20–25% for ligaments.
Here is the core of why it works. Ligaments and tendons have very poor blood supply. When they are torn, overstretched, or slowly worn down, the body's healing response is incomplete — some repair happens, but the tissue never quite returns to full strength. The result is a joint that remains unstable, pain generators that never fully switch off, and a chronic condition that rest and physiotherapy alone cannot reverse.
Prolotherapy interrupts this impasse. The dextrose creates a controlled, localised stimulus at the injection site — the body reads this as a repair call. Growth factors are released. Fibroblasts, the cells that synthesise collagen, are recruited. New collagen is laid down over a series of sessions, the tissue gradually regains its strength, and pain diminishes as the actual structural problem improves — rather than simply being chemically quietened.
Prolotherapy does not mask pain. It targets the structural weakness underneath — in ligaments, tendons, joint capsules, and nerve tissue — by stimulating the body to produce new collagen and repair what was damaged. This is regenerative medicine at its most accessible level.

I want to be straightforward with you: prolotherapy is not a treatment for every kind of pain. But its range of application is genuinely wide — and the evidence behind it is now strong enough that I use it with real confidence across the conditions below.
The most extensively studied use of prolotherapy. Multiple randomised controlled trials confirm that intra-articular dextrose injections reduce pain and improve knee function significantly — including in direct comparison against physiotherapy alone. A 2024 trial in the Journal of Orthopaedic Surgery and Research found that combining intra-articular prolotherapy with perineural injections produced particularly strong outcomes. For patients with mild to moderate knee osteoarthritis who are not yet ready for joint replacement — or simply do not want it — this is one of the best-evidenced non-surgical options available.
Ligaments are the strong fibrous bands that hold each joint in the correct position. When they are overstretched, partially torn, or gradually weakened over years, the joint loses stability and pain becomes persistent. The sacroiliac joint — the junction between the spine and the pelvis — is one of the most common overlooked sources of low back and buttock pain. Prolotherapy to the sacroiliac ligaments carries Level 1–2 evidence and produces excellent results in the right patient.
A 2024 systematic review of 20 randomised controlled trials covering 1,136 patients found prolotherapy effective for tendinopathy in 85% of included studies — with dextrose used in 95% of those trials. Tennis elbow (lateral epicondylitis), rotator cuff lesions, and plantar fasciitis were the most studied conditions. These are precisely the day-to-day injuries that accumulate quietly — the shoulder that has been sore since that one bad gym session six months ago, the heel that is agony for the first ten minutes every morning, the elbow that flares whenever work pressure peaks.
Back pain driven by facet joint degeneration, disc-related instability, or sacroiliac ligament laxity is another well-supported indication. Level 3 evidence across multiple study designs supports prolotherapy for axial low back pain — and in clinical practice, patients who have spent years cycling through anti-inflammatories often find genuine and lasting relief within a prolotherapy course.
Those tight, tender knots in the neck and shoulder that send pain shooting towards the head, or into the arm — trigger points — respond well to dilute dextrose injection, often alongside a small amount of local anaesthetic. This is especially effective in the paravertebral muscles, trapezius, and glutes. Hyderabad's working population carries a remarkable amount of postural tension in these areas, and trigger point prolotherapy can provide relief that no amount of heat pad or massage had achieved.
A 2024 case series in patients with hypermobile Ehlers-Danlos syndrome showed significant improvement in both pain and subluxation — partial dislocation — with dextrose prolotherapy. These patients are routinely told there is little that can be done short of reconstructive surgery. Prolotherapy does not deliver overnight joint tightening, but it steadily builds the structural scaffolding that reduces instability and pain over time.
Jaw pain, clicking, and limited mouth opening are common and notoriously hard to treat. A 2026 retrospective study of 66 patients with TMD that had not responded to conventional treatment found that hypertonic dextrose prolotherapy — sometimes with PDRN added — produced significant improvements in both pain and function after an average of just 2.3 sessions.
One of the most elegant uses of dextrose prolotherapy is in carpal tunnel syndrome (CTS) — the most common nerve entrapment condition, and one that is becoming increasingly prevalent across Hyderabad's office corridors. Wrists held in keyboard position for nine or ten hours a day, hands that never quite get a rest — these are the conditions in which the median nerve gets progressively compressed and tethered inside the narrow carpal tunnel in the wrist.
Here, the technique does two things simultaneously. A larger volume of 5% dextrose — typically 5 to 10 mL — is injected under real-time ultrasound guidance precisely around the median nerve. The fluid creates a hydraulic plane that physically separates the nerve from the adhesions and scar tissue trapping it: this is nerve hydrodissection, using fluid the way a careful engineer uses a thin tool to release something that has been jammed. At the same time, the dextrose quietens TRPV1 receptors on the nerve surface, reducing the release of Substance P and CGRP — the neurochemical messengers responsible for the burning, tingling, neuropathic pattern of CTS pain.
The evidence is now genuinely strong. A landmark double-blind RCT in Mayo Clinic Proceedings (Wu et al., 2017) showed perineural 5% dextrose superior to saline for pain, function, and nerve conduction at six months. A further RCT in Annals of Neurology (Wu et al., 2018) found dextrose statistically non-inferior to triamcinolone steroid — matching the gold-standard injectable without any steroid side effects. A 2025 meta-analysis in Archives of Physical Medicine and Rehabilitation confirmed comparable efficacy across the literature, recommending dextrose as a corticosteroid replacement. Volume matters: a 2024 RCT found 10 mL of D5W more effective than 5 mL for reducing nerve swelling at twelve weeks. And for patients who have already had carpal tunnel release surgery but remain in pain from post-operative scarring, perineural dextrose injection offers a meaningful non-surgical option — published case reports document pain scores dropping from 8 to 3 after a single session.
I want to step away from the clinical detail for a moment, because something important gets overlooked if I do not say it plainly.
The people who sit across from me at IBAP Clinics are not abstractions. They are real. The accountant in his forties with plantar fasciitis that spikes every rainy season when he stands on the hard office floor all morning. The software developer with her wrist aching by 4 p.m. every afternoon, telling herself it will ease once the sprint is over. The retired schoolteacher who still wants to do his daily 5 km walk but has quietly started cutting it to two because the hip protests. The homemaker who manages the household, the cooking, elderly in-laws, and children's school logistics — and mentions her knee pain almost in passing, as though it were a lesser concern. Young people grinding through coaching classes for entrance examinations, whose necks and shoulders have been in continuous tension for months. Middle-aged professionals who loved an evening at the cinema or a long Friday puja at the temple, who now quietly negotiate with their knees about what is worth attempting.
Pain is too often dismissed in Indian culture. Stoicism is admired — push through, it will pass, this is ageing, everyone has this. But chronic pain is not a moral failing. It is a signal from tissue that has been overwhelmed and not adequately repaired. And the body, given the right prompt, still has a remarkable capacity to fix itself.
Think of a damaged ligament the way you would think of an old suspension bridge whose cables have started to fray. Traffic still crosses — movement is still possible — but the cables have lost their original tension, and the structure sways with every load. You could close the bridge entirely and rebuild it from scratch. Or you could send in engineers to reinforce the existing cables, weaving fresh steel through the old, restoring the original strength without demolishing what remains. Prolotherapy is this second approach: targeted repair, working with what the body already has, rather than replacing it altogether.
— Dr. Vijay Bandikatla, IBAP ClinicsThe core solution is refreshingly straightforward: hypertonic dextrose diluted in sterile water, combined with a small amount of local anaesthetic — lignocaine or bupivacaine — to reduce discomfort on injection. But this is not a fixed recipe. Depending on the clinical picture, several adjuvants can be added or used alongside dextrose to enhance the result.
| Adjuvant | How It Works | Best Used For | Evidence Level |
|---|---|---|---|
| Hypertonic Dextrose (5–25%) | Osmotic stimulus → fibroblast activation → new collagen production | Ligaments, tendons, joints, trigger points, nerves | Level 1–2 |
| Platelet-Rich Plasma (PRP) | Concentrated growth factors (TGF-β, PDGF, VEGF) → accelerated repair | Tendon tears, knee OA, shoulder, nerve (CTS) | Level 1–2 |
| Polydeoxyribonucleotide (PDRN) | A2A receptor agonism → anti-inflammatory + cartilage/tendon repair | TMJ, cartilage, tendinopathy | Level 2–3 |
| Ozone (O3) | Oxidative burst → growth factor release + antimicrobial | Disc, intramuscular trigger points | Level 2–3 |
| Local Anaesthetic (Lignocaine / Bupivacaine) | Immediate comfort; carrier vehicle for dextrose | All injections as standard | Established practice |
| Mannitol | Osmotic agent; glucose-free alternative | Patients with poorly controlled diabetes | Emerging |
The combination I choose depends on who is sitting across from me. A competitive tennis player in their late twenties with a partially torn rotator cuff and strong healing capacity needs a different formula to a 65-year-old retired government officer with knee OA and reduced cartilage. For the former, dextrose with lignocaine is often perfectly sufficient. For the latter, I am more likely to combine dextrose with PRP — drawing on both the structural repair stimulus and the concentrated growth factor delivery that PRP provides. For someone with widespread myofascial trigger points across the paraspinal muscles after years of desk work, dilute dextrose with careful needling technique, or a small addition of ozone, is the better approach. Matching the solution to the situation is where clinical experience matters most.
| Treatment | What It Does | How Long It Lasts | Risks | Does It Repair? |
|---|---|---|---|---|
| Corticosteroid Injection | Suppresses inflammation | Weeks to months | Tendon weakening and tissue atrophy with repeat use | ❌ No |
| Hyaluronic Acid | Lubricates the joint temporarily | 3–6 months | Occasional post-injection flare | ⚠️ Partial |
| Prolotherapy (Dextrose) | Stimulates fibroblasts, builds new collagen | Long-lasting — months to years | Expected ache 24–72 hrs; well tolerated | ✅ Yes |
| PRP | Delivers concentrated growth factors | Long-lasting | Mild flare; rare infection | ✅ Yes |
| Surgery | Structural repair or replacement | Permanent when successful | Significant: anaesthetic, infection, recovery | ✅ Yes (invasive) |
The key distinction is this: steroids suppress the pain signal quickly, but do nothing for the tissue causing it — and repeated use can actively weaken the very tendons and cartilage you are trying to protect. Prolotherapy works more slowly, but it is working toward actual structural improvement. For patients in Hyderabad who are not ready for surgery and are understandably wary of long-term steroid dependence, it sits exactly where they need a treatment to be.
Every prolotherapy injection at IBAP Clinics is performed under real-time ultrasound guidance. Not occasionally — every time. Injecting into the wrong tissue plane achieves nothing, and without being able to see the needle tip at every moment, you are guessing rather than treating. I do not guess with patients.
Before: We review your imaging, examine the target area carefully, and map the injection sites. No general anaesthetic is needed. The procedure takes 20 to 45 minutes depending on how many sites are being treated.
During: An initial needle prick, then a deeper aching pressure as the dextrose enters the tissue. The local anaesthetic in the solution reduces this considerably. The sensation is the osmotic stimulus working — which is, in a sense, the entire point.
After: An ache, sometimes quite noticeable, for 24 to 72 hours. I tell every patient this in advance because it is not a complication — it is the repair response beginning. Simple paracetamol manages it well. What to avoid: any NSAID (ibuprofen, diclofenac, naproxen, nimesulide) for 72 hours either side of the injection. Taking an anti-inflammatory after prolotherapy is rather like turning off the generator the moment it starts running — it directly blunts the mechanism the treatment depends on.
Sessions are spaced 4 to 6 weeks apart. Most patients need 3 to 6 in total. Some notice a genuine shift after the first or second session. Others take longer. The body repairs on its own schedule, and patience is — genuinely — part of the process.
Avoid all NSAIDs — ibuprofen, naproxen, diclofenac, nimesulide — for at least 72 hours before and after each prolotherapy session. These medications directly suppress the inflammatory cascade that the injection is designed to activate. They reduce the benefit of the treatment.
Honesty here matters more than enthusiasm. Relative contraindications include active local infection, known allergy to any component of the solution, significant clotting disorders, and poorly controlled diabetes — though in most diabetic patients the glucose load from a standard session is small enough to be clinically irrelevant, and mannitol is available as an alternative. Prolotherapy should not be delivered over an acutely inflamed joint during a rheumatoid or gout flare.
It is also not a substitute for surgery where structural failure is complete — a fully ruptured tendon, a joint with almost no cartilage remaining. There are limits to what a regenerative stimulus can achieve when the tissue itself has gone. I will say this directly at consultation, rather than offer a treatment that is insufficient for your situation.
This is something I feel strongly about — not just clinical opinion but consistent clinical observation. Prolotherapy produces its best results when it is part of a coordinated approach, not a last resort tried after everything else. Combining it with targeted physiotherapy, adequate nutritional support (protein and micronutrients for collagen synthesis), postural correction, and sensible activity modification produces outcomes that injections alone cannot match.
Pain is rarely a purely mechanical problem with a purely mechanical solution. The patients who do best are those who engage with their own recovery — who show up to physiotherapy, who adjust the way they sit at their workstation, who take sleep seriously. I know that sounds demanding given the pace of life most of my patients are navigating. But the biology is clear: cortisol — the primary stress hormone — directly impairs collagen synthesis. A body in a state of chronic physiological overload cannot repair its connective tissue efficiently. The structural and the psychological genuinely answer to each other.
| Study / Source | Condition | Key Finding | Quality |
|---|---|---|---|
| Capotosto et al., 2024 — AJSM (20 RCTs, n=1,136) | Sports tendinopathy | Effective in 85% of studies; dextrose used in 95% of trials | Level 1 |
| Fu et al., 2024 — J Orthop Surg Res RCT | Knee osteoarthritis | Prolotherapy + perineural injection significantly superior to exercise alone | Level 1 |
| Ciftci et al., 2023 — Double-blind RCT (n=60) | Lateral epicondylitis (tennis elbow) | Both 5% and 15% dextrose superior to saline for pain and function | Level 1 |
| Wu et al., 2017 — Mayo Clin Proc RCT | Carpal tunnel syndrome | Perineural 5% dextrose superior to saline for pain, hand function, and NCS at 6 months | Level 1 |
| Wu et al., 2018 — Ann Neurol RCT | Carpal tunnel syndrome | 5% dextrose non-inferior to triamcinolone at 6 months; no steroid side effects | Level 1 |
| Oh et al., 2025 — Arch PM&R meta-analysis | Carpal tunnel syndrome | Dextrose comparable to corticosteroids; recommended as replacement option | Level 1 |
| Choi et al., 2026 — TMJ retrospective (n=66) | TMJ disorder | Significant improvement in pain and mouth opening; average 2.3 sessions needed | Level 3 |
| Hauser et al. — J Prolotherapy evidence review | Multiple MSK conditions | Level 1–2 evidence for OA, tendinopathy, sacroiliac pain, myofascial pain | Level 1–2 |
| Zhou et al., 2025 — PMC (IGF-2R mechanism) | Tendon injury | Dextrose acts via IGF-2R pathway; dose-dependent collagen improvement confirmed | Level 2–3 |
If you have been living with chronic joint, ligament, tendon, muscle or nerve pain and want a non-surgical path forward, we would like to hear from you. Book a consultation with Dr. Vijay Bandikatla at IBAP Clinics — Banjara Hills or Madeenaguda.
2nd Floor, 284/A, Road No. 12
Above IDFC First Bank, near Omega Hospitals
MLA Colony, Banjara Hills
Hyderabad 500034
Sy No. 2, 4th Floor, Plot No. 200
Beside South India Shopping Mall
Opp. Fortune Heights, Mythri Nagar
Madeenaguda, Hyderabad 500049
This article is for general patient education and informational purposes only. It does not constitute medical advice and should not replace a professional consultation with a qualified pain specialist. Prolotherapy and related interventions must be individually assessed and performed by an appropriately trained clinician. Results vary between patients. Always seek the advice of your doctor or other qualified health professional with any questions regarding a medical condition or treatment. Dr. Vijay Bandikatla and IBAP Clinics accept no liability for any decision taken on the basis of this content alone.


