Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
A plain-language clinical guide by Dr Vijay Bhaskar Bandikatla — covering the cells, the technique, cartilage regeneration, tendon healing, AVN of the hip, the legal landscape, and when to combine with PRP.
Patients come to me having read about BMAC online — and half of them arrive with wild expectations, and the other half with wild fears. Some think I am going to inject magical stem cells that will regrow their knee cartilage overnight. Others are convinced it is some experimental, illegal procedure borrowed from science fiction. The truth, as with most things in medicine, sits somewhere more nuanced and — actually — more interesting than either of those stories.
BMAC stands for Bone Marrow Aspirate Concentrate. At its most basic, it is this: we take a small amount of your own bone marrow, typically from the back of your pelvic bone, spin it in a specialised centrifuge to concentrate the most valuable cellular components, and then inject that concentrate directly into the area that needs healing — a joint, a tendon, a necrotic bone. Same day. Your own tissue. No donors. No genetic modification. No laboratory culture.
That is the procedure in one paragraph. But what makes it remarkable — and why it has become one of the most actively researched areas in regenerative pain medicine — is what those concentrated cells actually do once they arrive at the target tissue.
BMAC works primarily through paracrine signalling — the injected cells release growth factors, anti-inflammatory cytokines, and signalling molecules that recruit the body's own repair machinery. It is less about the cells themselves replicating, and more about them acting as a biological trigger. Think of BMAC not as a builder, but as the foreman who arrives on site and organises the construction crew.
This is the part of any BMAC consultation I spend the most time on. Because the term "stem cells" gets thrown around loosely — by clinics, by patients who have googled, and frankly by some doctors who should know better. So let us be precise.
When bone marrow is aspirated and concentrated, you get a heterogeneous mixture of nucleated cells. Nucleated simply means cells with an intact nucleus — as opposed to red blood cells, which lose their nucleus at maturity. The key populations in BMAC include:
These are the cells that everybody is really talking about when they say "stem cells" in the orthopaedic or pain context. MSCs have the ability to differentiate — under the right conditions — into bone cells (osteoblasts), cartilage cells (chondrocytes), fat cells (adipocytes), and muscle cells. Critically, they also secrete a rich cocktail of growth factors and cytokines. In raw bone marrow, MSCs are present at roughly 0.001–0.01% of all nucleated cells — an extraordinarily low concentration. Concentrating the aspirate raises this, but BMAC is not a pure MSC product. This matters hugely from a regulatory standpoint, as I will explain shortly.
These are the cells responsible for generating blood cell lines. While not directly involved in orthopaedic regeneration, they contribute to the immune-modulatory environment post-injection, helping to damp down the local inflammatory response.
BMAC concentrate is platelet-rich. These platelets carry growth factors — PDGF, TGF-β, VEGF, IGF-1 — that directly stimulate tissue repair. In this sense, BMAC already has PRP-like properties built in, which is one reason even standalone BMAC can produce meaningful results.
The aspirate contains a symphony of interleukins and other signalling proteins — some anti-inflammatory, some pro-regenerative — that help modulate the local tissue environment. In an arthritic joint, for instance, BMAC can reduce the levels of destructive metalloproteinases and inflammatory cytokines that are slowly eating away at cartilage.
Think of BMAC as sending an emergency response team to a damaged building. The MSCs are the architects — they can theoretically rebuild structural components like cartilage or bone. The growth factors are the raw materials. The cytokines are the safety officers — clearing out the chaos so meaningful work can begin. No single member of the team does everything. But together, they shift the local environment from destruction to repair. That shift is what we are buying when we use BMAC.
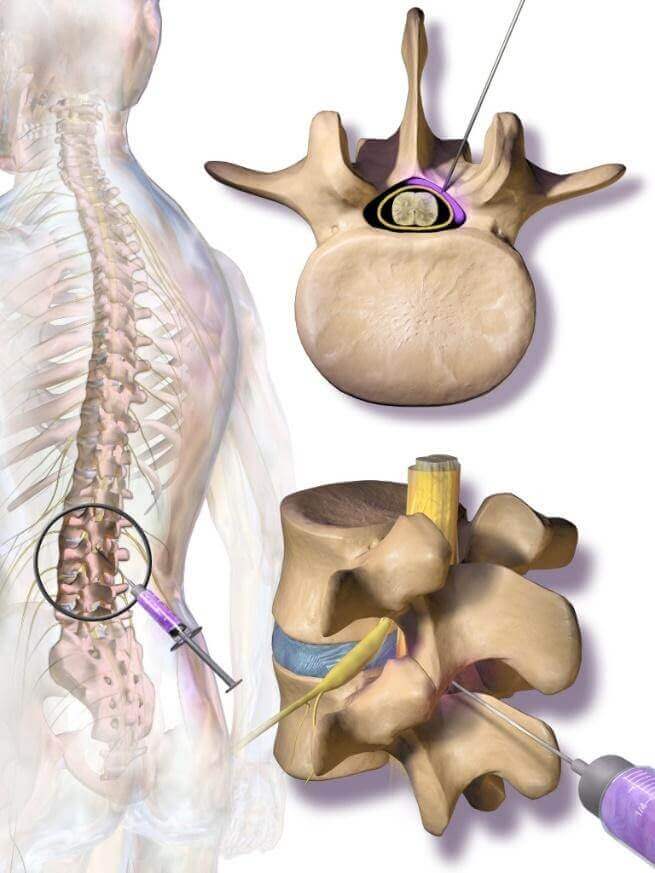
The posterior iliac crest — the curved ridge at the back of your hip bone — is the workhorse site for BMAC harvesting, and for good reason. It is easily accessible, yields the highest density of progenitor cells in the adult skeleton, and carries minimal morbidity when handled properly.
The procedure begins with the patient lying prone or in a lateral decubitus position. The skin and periosteum over the iliac crest is infiltrated with local anaesthetic — this is the most uncomfortable part, honestly, the pressure sensation of the needle entering bone. A large-bore harvest needle (typically 8–11 gauge) is then inserted through a small stab incision into the medullary cavity of the iliac bone. Bone marrow is aspirated in multiple small aliquots — usually 2–3 ml per pull, from different depths and angles — to maximise cellular diversity and avoid dilution with peripheral blood. Total aspirate volume is typically 40–80 ml.
The aspirate is then transferred to a dedicated processing kit and centrifuged in a closed, point-of-care system — the Arthrex Angel, the Harvest SmartPReP, or similar platforms are common. Centrifugation separates the cellular layers by density, allowing selective concentration of the nucleated cell-rich fraction. The result is 6–10 ml of BMAC that is then drawn into syringes for injection.
The anterior iliac crest can also be used — useful when the patient cannot tolerate prone positioning. Tibial and calcaneal marrow has been used in foot and ankle applications. The iliac crest remains standard because of its superior yield.
SVG DIAGRAMI want to be very direct about this, because it matters — clinically, ethically, and legally. BMAC is not the same as stem cell therapy, even though it contains cells with stem-cell-like properties. The distinction is not just semantic. It is the difference between what you can legally and ethically do in a clinic today and what requires regulatory approval.
Mesenchymal stromal cells (MSCs) in BMAC are present at very low concentrations and are not culture-expanded — they are used exactly as nature intended, in their native marrow environment, with their supporting cell populations and signalling molecules intact. The moment you take those cells out, grow them in a laboratory for two to four weeks, expand them to millions, and re-infuse them — that is stem cell therapy. That is a drug in the regulatory sense, and in India, that requires CDSCO approval.
The regulatory landscape in India has been in evolution. The ICMR and DBT established stem cell guidelines in 2007, with revisions in 2017 through the National Guidelines for Stem Cell Research (NGSCR). Importantly, the two-tier oversight structure — the IC-SCR and NAC-SCRT — was dissolved in March 2024, creating a regulatory transition period. Under the Drugs & Cosmetics Act 1940 as applied to cellular therapies: minimally manipulated, autologous, same-day, homologous use is generally permissible without CDSCO drug approval. This is the category BMAC falls into. Cells that are substantially manipulated — culture-expanded, genetically modified, combined with biomaterials for non-homologous use — are regulated as drugs and require full regulatory clearance.
So when I perform BMAC at IBAP Clinics, I am working within this framework: autologous (your own cells), minimally manipulated (concentrated but not cultured), same-day (no storage or banking), and homologous (bone marrow cells being used for bone and connective tissue indications). This is the ethical safe harbour.
In the United States, the FDA classifies human cells, tissues, and cellular and tissue-based products (HCT/Ps) under 21 CFR Part 1271. Same-day, minimally manipulated, autologous BMAC generally qualifies for a Section 361 exemption — meaning it does not require pre-market approval. Cultured, expanded, or allogeneic cell products require an Investigational New Drug (IND) application and full clinical trial approval. Many US orthopaedic and sports medicine practitioners routinely use point-of-care BMAC under this framework.
Cartilage is notoriously bad at healing itself. It has no blood supply, no nerve supply, and very few resident cells. Once it is damaged or worn away, the body struggles enormously to replace it. This is why joint replacement surgery has become so common — once cartilage is gone beyond a certain threshold, there are limited options. BMAC is the most compelling biological strategy we currently have for addressing early-to-moderate cartilage loss. And I will be careful to say "addressing" rather than "reversing," because that is a more honest word.
What BMAC does to cartilage — specifically in knee osteoarthritis, which has the largest evidence base — is reduce the inflammatory cytokine load that accelerates cartilage breakdown, provide MSC-derived signals that can stimulate chondrocyte activity, and improve the subchondral bone environment that cartilage sits upon. Several studies have now shown MRI-measurable improvements in cartilage thickness and quality at the 12–24 month mark. The 2025 narrative review in a peer-reviewed journal (PMC12113016) affirmed BMAC's promise for cartilage repair and subchondral bone remodelling, though it rightly called for larger randomised controlled trials. A 2024 four-year follow-up study on KL Grade III–IV knee OA (Nature Scientific Reports, Graz) showed sustained pain reduction and functional improvement — not perfect cartilage, but meaningful preservation and symptom relief.
The critical caveat: the window for BMAC benefit is earlier disease. Grade IV osteoarthritis with bone-on-bone contact is unlikely to respond meaningfully. Grade II–III disease, with cartilage loss but intact bone surfaces — that is where the evidence is strongest, and where I would consider BMAC as a serious non-surgical option.
EVIDENCE TABLE| Condition | Evidence Level | Key Finding | Notes |
|---|---|---|---|
| Knee OA (Grade II–III) | Level II–III | Comparable to viscosupplementation at 24 months; superior in cartilage metrics | Jeyaraman et al, Indian J Orthop 2024 |
| Knee OA (Grade III–IV) | Level III | 4-year sustained benefit in pain and function; no TKA at follow-up in majority | Graz study, Sci Rep 2024 |
| AVN Femoral Head (pre-collapse) | Level II–III | Core decompression + BMAC delays collapse and reduces THA need | Pawar et al scoping review; Erciyes et al 2025 |
| ACL Reconstruction | Level I (RCT) | BMAC augmentation improved IKDC scores and graft integrity on MRI | Systematic review, PMC11703946 2025 |
| Rotator Cuff Partial Tear | Level II–III | BMAC + PRP superior to exercise at 3 months on VAS and ASES | Kim et al, J Orthop Surg 2018 |
| Partial Meniscectomy (early OA) | Level I (RCT) | Significantly improved early knee OA outcomes vs control at 24 months | Yanke et al, Am J Sports Med 2024 |
Avascular necrosis of the femoral head — AVN — is devastatingly common in India, and I say this from years of clinical practice. The causes are well-known: prolonged corticosteroid use (often for rheumatoid arthritis, lupus, or even the aftermath of post-COVID treatment), excessive alcohol consumption, trauma to the hip. India has a particular burden of post-COVID AVN that we are still navigating — a legacy of the heavy steroid protocols used in 2020–2021.
AVN at its core is a problem of blood supply failure to the femoral head. The bone dies, and without intervention, the head collapses. Once collapse occurs, the options narrow sharply to hip replacement. The challenge — and the opportunity — is the pre-collapse stage.
Core decompression with BMAC injection directly into the necrotic lesion is the most evidence-supported joint-preserving strategy for early-stage AVN. The core decompression — drilling a channel into the femoral head — reduces the elevated intraosseous pressure that worsens ischaemia. BMAC then provides the osteogenic (bone-forming) cellular signals and growth factors needed to stimulate revascularisation and bone regeneration within the necrotic zone.
A 2025 prospective study (Medicine Journal, Erciyes et al.) of 22 patients with pre-collapse AVN demonstrated that core decompression with BMAC injection produced meaningful clinical and radiological improvement at 12-month follow-up, with reduced progression rates compared to historical decompression-only data. A 2021 scoping review analysing 612 hips across 11 studies confirmed benefit in precollapse stages in reducing radiological progression and hip replacement rates.
My approach at IBAP Clinics is to combine core decompression with BMAC and often add a biological cocktail — which may include PRP and concentrated growth factors — to maximise the regenerative signal. We use fluoroscopic guidance to target the concentrate precisely into the necrotic zone, not just the decompression track. This precision matters. You are trying to deliver cells to a defined area of ischaemic bone, not flood the joint.
Beyond joints, BMAC has found an increasingly important role in soft-tissue injuries. Tendons, in particular, have poor intrinsic healing capacity — partly because of their limited vascularity, and partly because the mechanical environment of repeated loading prevents the orderly collagen deposition that proper healing requires. Rotator cuff tears, Achilles tendinopathy, lateral epicondylitis, gluteal tendinopathy, patellar tendinopathy — these are conditions where conventional physiotherapy and steroid injections often give partial, temporary relief at best.
BMAC's MSC content can differentiate into tenocytes (tendon cells) under the right biochemical cues. More importantly, the growth factor payload — particularly TGF-β and PDGF — directly stimulates collagen synthesis and tendon matrix remodelling. In a systematic review of BMAC in tendon pathology (PMC5632955), multiple preclinical and early clinical studies confirmed improved tendon integrity and reduced re-tear rates with BMAC augmentation, particularly in rotator cuff repair.
For significant muscle tears — Grade II–III hamstring tears in athletes, for example — BMAC injected at the zone of injury provides both anti-inflammatory and regenerative signals. The myogenic differentiation potential of MSCs, combined with the growth factor milieu, can accelerate organised muscle fibre regeneration. Clinical evidence here is less robust than for joints, but the biological rationale is sound, and outcomes in sports medicine practices have been encouraging.
COMPARISON TABLE| Property | BMAC | PRP | Corticosteroid |
|---|---|---|---|
| Contains regenerative cells | ✓ MSCs + progenitors | ✗ | ✗ |
| Anti-inflammatory effect | ✓ (cytokine modulation) | ~ Modest | ✓ Strong, short-term |
| Structural repair potential | ✓ High | ~ Low-moderate | ✗ None |
| Cartilage disease-modifying | ✓ | ~ Possibly short-term | ✗ May worsen |
| Procedure complexity | Moderate (harvest + inject) | Low (blood draw + inject) | Very low (inject only) |
| Cost | High | Moderate | Low |
| Duration of effect | 12–24+ months | 3–6 months typically | 4–12 weeks |
| Tissue damage risk (long-term) | ✓ None known | ✓ None known | ✗ Yes (repeated use) |
I think of BMAC and PRP as complementary rather than competing. PRP — platelet-rich plasma — is rich in growth factors and creates what I call the "landing pad." It activates the local environment, stimulates cell recruitment, and begins the growth factor cascade. BMAC then delivers the cellular reinforcements — the MSCs and progenitor cells that can actually drive structural regeneration.
A 2024 systematic review and meta-analysis (PMC11416799) specifically comparing BMAC alone versus BMAC with PRP in rotator cuff repair found growing interest in the combined modality, though consensus on the optimal protocol has not yet been established. In AVN, BMAC combined with growth factor concentrates — sometimes including PRP — is becoming the standard in leading regenerative centres.
My sequencing preference: PRP is injected at the target site first, either a few minutes before BMAC or simultaneously. The rationale is that PRP degranulates immediately upon activation, flooding the area with growth factors that signal to incoming cells. The BMAC is then delivered into this prepared environment, where its cellular cargo has the optimal conditions to engraft, survive, and function. Think of PRP as preparing the soil and BMAC as planting the seeds.
Patient selection is perhaps the most critical determinant of outcomes with BMAC. The procedure is not appropriate for every patient with joint pain, and setting realistic expectations is as important as the technical execution. These are the patients in whom I find BMAC most rewarding:
Patients with early-to-moderate joint degeneration — OA Grade II–III — who have not responded adequately to physiotherapy, weight management, and oral treatments, and are not yet appropriate for or willing to consider joint replacement. Younger patients — particularly those under 55–60 — where buying five to ten years of reasonable joint function before any surgical conversation is enormously valuable. Patients with AVN of the femoral head at pre-collapse stage (Ficat I–IIb), where BMAC combined with core decompression may genuinely avert hip replacement. Athletes and active individuals with tendon or ligament injuries where the goal is structural healing, not just symptom management. And patients who have already had surgery and are looking for biological augmentation of healing — post-ACL reconstruction, post-rotator cuff repair.
Patients who are not likely to benefit: those with end-stage disease and complete cartilage loss, systemic inflammatory conditions that have not been adequately controlled, active joint infection, malignancy, or bleeding disorders. Haematological bone marrow conditions also preclude harvest.
I have been practicing pain medicine in Hyderabad for nearly eight years now, having spent the earlier part of my career in the NHS. And one thing strikes me every single week in clinic: the Indian musculoskeletal burden is uniquely heavy, and it is getting worse.
We see young IT professionals — 28, 32 years old — with knee pain from being sedentary at desks for twelve hours a day. We see builders and factory workers whose joints have simply been worn beyond what the human body was designed to endure. We see patients who tried to manage their joint pain with years of NSAIDs and have now added stomach damage to their joint damage. The potholes on the roads, the brutal speeds at which we take those speed breakers, the weight carried on two-wheelers — these are not trivial mechanical stresses on the spine and hips over a lifetime of daily commuting.
And then there is the steroid legacy. So many patients coming to me with AVN or fragility fractures have a history of poorly supervised steroid prescribing — for everything from allergies to back pain. The post-COVID cohort has added substantially to this. These are young patients, often in their 30s and 40s, facing femoral head collapse and the prospect of hip replacement decades too early.
This is the context in which I believe BMAC and regenerative medicine have a genuinely transformative role to play in India. Not as a luxury treatment for the wealthy, but as a serious, evidence-based attempt to give patients their lives back without surgery. The cost remains a barrier — I will not pretend otherwise. But as the evidence strengthens and technology becomes more accessible, the calculus will shift.
Pain is not just a sensation. It is a story — of years of posture, of work, of stress, of how you have used and perhaps overused your body. When I inject BMAC, I am not just treating a knee or a hip. I am trying to give that patient back the mobility to walk their daughter to school, or return to their morning walk in KBR Park, or play cricket in the colony on Sunday morning. The biology is important. But the reason we do it — that is the part that matters most.
Whether it is knee osteoarthritis, hip AVN, a stubborn tendon injury, or post-surgical healing — let us have a proper clinical conversation about whether regenerative medicine is the right path for you.
2nd Floor, 284/A, Road No. 12
Above IDFC First Bank
Near Omega Hospitals, MLA Colony
Banjara Hills, Hyderabad – 500034
Sy No. 2, 4th Floor, Plot No. 200
Beside South India Shopping Mall
Opp. Fortune Heights, Mythri Nagar
Madeenaguda, Hyderabad – 500049
This article has been authored by Dr Vijay Bhaskar Bandikatla MBBS DA FRCA FFPMRCA and is intended for general patient education and informational purposes only. It does not constitute personalised medical advice, a clinical diagnosis, or a treatment recommendation. BMAC and other regenerative medicine procedures carry procedural risks and are not appropriate for every patient or every condition. Outcomes vary depending on patient selection, disease stage, comorbidities, and procedural technique. Individual outcomes cannot be guaranteed. The regulatory information provided reflects the position as understood at the time of publication and may be subject to change. Patients should seek direct consultation with a qualified pain medicine or orthopaedic specialist before making any treatment decisions. IBAP Clinics — Vijay Advanced Pain Clinics Pvt. Ltd. — operates in compliance with Indian medical law and ethical guidelines.
EXCELLENTTrustindex verifies that the original source of the review is Google. Good pain relief with treatmentPosted on GoogleTrustindex verifies that the original source of the review is Google. Best for pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. बहुत अच्छा लगा हमें ये ट्रिटमेंट करा के अच्छे डॉक्टर और अच्छे स्टाफ हैं और काम पैसे में अच्छा अच्छा ट्रिटमेंट होता हैPosted on GoogleTrustindex verifies that the original source of the review is Google. Very nice, good and helpful staf, overall good experiencePosted on GoogleTrustindex verifies that the original source of the review is Google. Very good doctors and good tritment Thank you doctorPosted on GoogleTrustindex verifies that the original source of the review is Google. One of the best clinic for the relief of back painPosted on GoogleTrustindex verifies that the original source of the review is Google. Very good treatment indo british clinic for every pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. I have visited indo british pain clinic this is superb clinic for pain relief that's why I have given 5 start rating to this clinic ...Posted on GoogleTrustindex verifies that the original source of the review is Google. My name is Raja Sekhar Reddy Tummuri from kakinada city My father was suffering nervous pain from last 3 years … I have decided to join with this op … Now everything fine after treatment done from DR. vijay sir … Wonderful service received from INDO British advanced pain clinic Hospitals in Hyderabad @ Banjara Hills road no 12.. Each and every staff response , concern , support & everything it’s too good Thank you so much … Special thanks to Mr. DR. Vijay bhaskar Bandi Katla …👏🏻👏🏻👏🏻👏🏻🙏🙏Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more

Founder & Interventional Pain Specialist — IBAP Clinics, Hyderabad
MBBS · DA · FRCA (London) · FFPMRCA (Pain Medicine, UK) · MBA (Hospital Management)
CCT (Anaesthesia & Pain Medicine, UK) · Advanced Pain Training (Cambridge University Hospitals)
DDSMed Sports Medicine (Chicago) · Fellowship in Neuromodulation & Advanced Pain (London)
Dr Vijay brings over 15 years of postgraduate training across the United Kingdom’s most prestigious institutions — including the Royal College of Anaesthetists, Cambridge University Hospitals, and a dedicated neuromodulation fellowship in London — to his practice in Hyderabad. He is one of very few clinicians in India trained to the level of FFPMRCA — the Faculty of Pain Medicine of the Royal College of Anaesthetists — the highest qualification in pain medicine available in the UK.
His specialist expertise spans the full spectrum of knee pain management: from precision PRP and BMAC injections to cooled radiofrequency genicular nerve ablation, intrathecal drug delivery, and spinal cord stimulation for refractory pain states. He manages cases ranging from the weekend cricketer’s torn meniscus to the elderly cardiac patient with end-stage OA who has been told there are no further options.
Home » Procedures » Bone Marrow Aspirate Concentrte (BMAC stem Cells)

In our pain clinic, we provide pain relief so you can regain your identity.
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us