Helpline :
9807 55 6789
- Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
A complete guide to activated protein serums, plasma lysates, conditioned serums, and the growing family of growth factor preparations — what they are, how they differ, and where they fit in modern regenerative pain medicine.
Let me start with a thought experiment. Imagine you are trying to renovate a damaged building — crumbling walls, broken scaffolding, structural cracks that have been there so long nobody even notices them anymore. You could bring in raw materials and hope the workers figure it out. Or you could bring in a specialist foreman with a precise briefing — specific instructions, exactly the right tools, delivered exactly where the damage is worst.
That, in essence, is the difference between general blood-derived therapies and growth factor concentrates. We have known for decades that the body contains its own repair machinery. What regenerative medicine has been steadily learning is how to isolate, concentrate, and deliver the specific molecular signals within that machinery — with far greater precision than a decade ago.
Growth factor concentrates (GFCs) are biological preparations derived primarily from autologous (your own) blood or tissue, processed to enrich specific proteins: growth factors, cytokines, anti-inflammatory mediators, and in newer preparations, extracellular vesicles. Unlike PRP — which captures a broad mixture of platelet contents — many GFC preparations can be selectively enriched for specific therapeutic molecules. Some are designed to maximise anabolic signalling. Others are engineered to block the very inflammatory proteins that drive cartilage destruction. Some do both simultaneously.
This is not merely a refinement of PRP. In several cases it represents a fundamentally different biological intervention — targeting specific pathological mechanisms rather than broadly stimulating repair.
The human body already contains every growth factor needed to repair itself. The challenge in chronic degenerative disease is not that these molecules are absent — it is that their concentrations at the site of damage are insufficient, their signals are overwhelmed by pro-inflammatory noise, or the tissue has lost its capacity to respond to them. Growth factor concentrates address all three of these problems simultaneously, each in a slightly different way depending on the preparation type.
Before we explore the different types of concentrate, it is worth understanding the key players. These proteins are not interchangeable. Each has a distinct receptor, a distinct cellular target, and a distinct therapeutic effect. Knowing this helps explain why different GFC preparations are suited to different clinical problems.
| Growth Factor / Cytokine | Primary Source | Key Biological Action | Therapeutic Relevance |
|---|---|---|---|
| IGF-1 (Insulin-like Growth Factor-1) | Platelets, liver, serum | Stimulates chondrocyte proliferation and proteoglycan synthesis; anti-apoptotic | Cartilage protection in OA; disc regeneration |
| TGF-β1 (Transforming Growth Factor-β1) | Platelets, bone matrix | Collagen synthesis, chondrogenesis, stem cell recruitment; dual pro/anti-inflammatory depending on context | Tendon repair, cartilage matrix production, fibrosis (at high dose) |
| PDGF (Platelet-Derived Growth Factor) | Platelets, macrophages | Cell proliferation, angiogenesis, fibroblast activation | Tendon and ligament repair; wound healing |
| VEGF (Vascular Endothelial Growth Factor) | Platelets, hypoxic tissue | New blood vessel formation; endothelial cell migration | Hypovascular tissue repair (tendons, menisci) |
| FGF-2 (Fibroblast Growth Factor-2) | Platelets, fibroblasts | Proliferation of fibroblasts, chondrocytes, muscle cells; angiogenesis | Cartilage repair, muscle regeneration |
| BMP-7 (Bone Morphogenetic Protein-7) | Bone, cartilage | Chondrogenesis, osteogenesis; counteracts catabolic IL-1 signalling in cartilage | Cartilage regeneration; intervertebral disc repair |
| IL-1Ra (Interleukin-1 Receptor Antagonist) | Monocytes / white blood cells | Competes with IL-1β for receptor binding; blocks cartilage breakdown cascade | Core therapeutic target in OA — specific to ACS/Orthokine and APS |
| sTNFRI / sTNFRII (Soluble TNF Receptors) | White blood cells | Bind and neutralise TNF-α, a key driver of joint inflammation | Specific to APS — anti-inflammatory in advanced OA |
| EGF (Epidermal Growth Factor) | Platelets, saliva, urine | Cell proliferation and differentiation; wound closure | Soft tissue repair; skin and connective tissue |
| HGF (Hepatocyte Growth Factor) | Platelets, fibroblasts | Anti-fibrotic; anti-apoptotic; regeneration of multiple tissue types | Emerging — disc and cartilage applications |
What this table illustrates is something important — and something that experienced regenerative clinicians appreciate deeply. No single growth factor is sufficient. Tissue repair requires a coordinated, temporally sequenced cascade of signals. The art of selecting a GFC preparation lies in matching the dominant therapeutic protein profile to the specific pathological process you are trying to reverse.
Blood is processed through a special concentrating device that selectively enriches both white blood cell proteins (IL-1Ra, sTNFRI, sTNFRII) and platelet-derived anabolic factors (IGF-1, TGF-β). The result: 3–10× higher anti-inflammatory cytokine concentrations than standard PRP, alongside significant growth factor enrichment. Single-injection protocol. Particularly suited to knee OA.
Whole blood is incubated with chromium sulphate-coated glass beads for 6–9 hours at 37°C. This stimulates monocytes to produce large quantities of IL-1Ra — the body's natural blocker of the IL-1β inflammatory cascade. Serum is then spun and used fresh or frozen. Multiple RCTs support its use in knee OA and lumbar radiculopathy. Associated with the treatment of elite athletes.
PRP is subjected to repeated freeze-thaw cycles (−80°C to +37°C) that rupture platelet membranes, releasing all intracellular growth factors into the surrounding plasma. The resulting cell-free solution is rich in growth factors without intact platelets — no inflammatory burst, sustained biological activity. Used in tendon, ligament, and intervertebral disc applications. Also the basis for many tissue engineering scaffolds.
A second-spin preparation that concentrates the plasma fraction rather than just the platelet layer, achieving higher concentrations of serum-borne growth factors including IGF-1, TGF-β, and FGF. Less inflammatory than LR-PRP due to the relative absence of leucocytes, but with a broader growth factor profile than simple plasma. Used in facial regeneration and early musculoskeletal trials.
Exosomes are nanoscale vesicles (30–150 nm) secreted by stem cells that carry growth factors, microRNAs, and signalling proteins across cell membranes. MSC-derived exosome preparations represent the frontier of cell-free regenerative medicine — achieving intercellular communication and epigenetic modulation without requiring live cell transplantation. Currently in advanced clinical trials for cartilage and disc regeneration.
Laboratory-produced versions of specific human growth factors in highly purified, concentrated form. rh-BMP-2 is already approved for spinal fusion and fracture repair. rh-PDGF (GEM 21S®) is approved for periodontal regeneration. While more expensive and not autologous, they offer reproducible dosing — a significant advantage over variable blood-derived preparations.
If I were to choose one growth factor concentrate to highlight as genuinely paradigm-shifting, it would be Activated Protein Serum — commercially known as nSTRIDE APS. Not because of marketing, but because of what it does biologically that nothing else achieves in a single preparation.
The fundamental problem in osteoarthritis — particularly knee OA, which affects enormous numbers of our patients in Hyderabad, from IT professionals whose knees have stiffened over years of sedentary desk work to older adults whose joints have taken the accumulated punishment of decades on uneven footpaths and overcrowded buses — is a tug-of-war between destruction and repair. Interleukin-1 beta (IL-1β) and TNF-α are the primary villains driving cartilage matrix breakdown. The body naturally produces antagonists to these molecules — IL-1Ra, sTNFRI, sTNFRII — but their concentrations in a diseased joint are simply overwhelmed by the inflammatory tide.
APS addresses this directly. The nSTRIDE processing system concentrates both the anabolic growth factors from platelets (IGF-1 up to 6.5× baseline, TGF-β up to 2.7× baseline) and the anti-inflammatory proteins from white blood cells (IL-1Ra up to 140× baseline, sTNFRI up to 18× baseline). One preparation. Two simultaneous mechanisms. Repair signals amplified, inflammatory signals suppressed.
The phase IIb randomised controlled trial by Kon et al. (2018) demonstrated significant and durable pain relief at twelve months following a single APS injection, with WOMAC scores substantially superior to saline. A subsequent multi-centre study confirmed these findings. The single-injection protocol is itself a practical advantage — for busy working professionals, for older patients who find repeat clinic visits difficult, and for those with needle anxiety, completing the biological course in one sitting matters enormously.
Autologous Conditioned Serum, available as Orthokine or Regenokine, takes a more focused approach: it is specifically designed to maximise IL-1Ra production. Whole blood is collected and incubated in tubes coated with chromium sulphate-treated glass beads, which activate monocytes — the immune cells responsible for producing IL-1Ra in the first place. Over six to nine hours at body temperature, these activated monocytes produce substantially elevated quantities of IL-1Ra, which is then harvested in the conditioned serum.
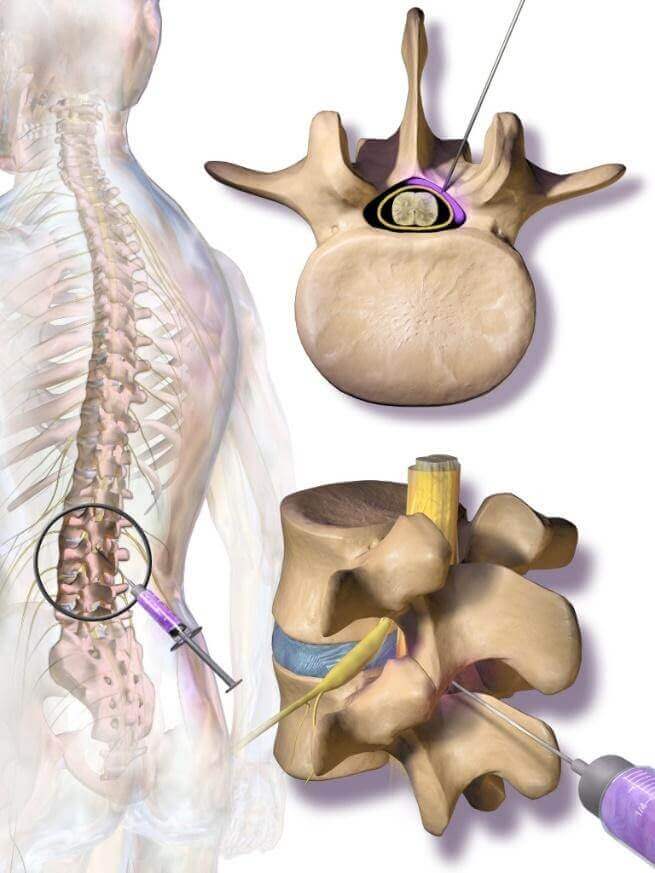
The resulting serum is typically administered as a series of six injections over three weeks — a more involved protocol than APS but one that has a longer evidence history and a particularly well-studied track record in lumbar radiculopathy, where ACS injected periradicularly (around the inflamed nerve root) has shown meaningful pain reduction in several trials including a robust German multicentre study.
Think of IL-1β as a fire alarm that has gone off inside your joint and won't switch off. The normal fire alarm reset button — IL-1Ra — is there, but too weak to reach it in the noise. ACS fills the room with enough IL-1Ra to finally press that button and silence the alarm. It doesn't rebuild the building. But it stops the destruction long enough for the remaining repair systems to work. That is still enormously valuable.
This is a preparation that does not get nearly enough attention in mainstream regenerative medicine discussions in India, and I think that is a gap worth addressing.
When intact platelets are injected as PRP, they activate upon contact with the tissue environment and degranulate — releasing all their contents simultaneously. This creates the immediate inflammatory burst that characterises PRP therapy: the three to five days of soreness, swelling, warmth. For tendons and ligaments, this acute signal is part of the therapeutic mechanism. For certain other applications — particularly intervertebral disc treatment, where the nucleus pulposus is an immune-privileged environment with very limited tolerance for inflammatory stimulation, or for use in cell culture scaffolds and tissue engineering — this inflammatory burst is actually a problem.
Plasma lysate solves this elegantly. By freeze-thawing PRP repeatedly at −80°C, platelet membranes are disrupted and all intracellular growth factors are released into the surrounding plasma. The result is a cell-free growth factor solution: rich in IGF-1, TGF-β, PDGF, FGF, and VEGF, but with no intact platelet membranes to trigger an acute inflammatory reaction. The growth factor activity is more sustained and the biological delivery is gentler.
In clinical practice, platelet lysates have their most compelling application in intradiscal regeneration protocols — where we inject into the nucleus pulposus or annulus fibrosus to attempt biological modulation of degenerative disc disease — and in peritendinous applications where tendon sheath inflammation from an acute platelet burst could cause more harm than good. They are also used extensively in tissue engineering and cell therapy laboratories as culture medium supplements, which is why the science behind them is considerably more advanced than most clinicians appreciate.
Let me be honest with you about this, because the internet is full of exaggerated claims and I believe patients deserve straight talking.
Cartilage is one of the most challenging tissues in the human body to regenerate. It has no blood supply of its own. It has no nerve supply. Its cells — chondrocytes — sit in lacunae within a dense extracellular matrix and have a very limited capacity to divide and migrate. When cartilage is damaged, the default response is not regeneration but fibrosis — formation of inferior fibrocartilage that looks somewhat like cartilage but does not function like it. This is why arthritis is progressive and why, in its end stages, it has historically required joint replacement.
Growth factor concentrates — particularly those rich in IGF-1, TGF-β, BMP-7, and FGF — have demonstrated genuine chondroprotective and in some contexts chondrogenic effects. IGF-1 reduces chondrocyte apoptosis (programmed cell death) and stimulates the production of type II collagen and aggrecan — the structural proteins that give cartilage its load-bearing properties. BMP-7 directly counteracts IL-1β-mediated cartilage matrix degradation. TGF-β promotes chondrogenic differentiation of mesenchymal stem cells — particularly relevant when combined with BMAC.
Growth factor concentrates can genuinely slow cartilage degradation, reduce inflammatory damage to existing cartilage, stimulate limited fibrocartilage repair, and in the best cases — particularly in early disease with good baseline cartilage stock — produce measurable increases in cartilage thickness on MRI over 12–24 months. They cannot regrow cartilage that is absent. The patient with bone-on-bone Kellgren-Lawrence grade IV arthritis needs a different conversation — one about joint replacement or high tibial osteotomy — not false hope about biological repair. Honest patient selection is not a limitation of regenerative medicine. It is its ethical foundation.
The most promising clinical signals for cartilage regeneration come from combination protocols: GFC (APS or platelet lysate) combined with BMAC-derived mesenchymal stem cells, delivered under ultrasound guidance, with structured rehabilitation afterwards. In patients with KL grade II or early grade III knee OA, we have seen reproducible improvements in cartilage quality on delayed gadolinium-enhanced MRI (dGEMRIC), alongside pain and functional improvements that persist beyond eighteen months in a meaningful proportion of cases.
If cartilage is the hard problem of regenerative medicine, tendon and ligament repair is where growth factor concentrates have produced their most consistently impressive clinical results — and where the biological rationale is perhaps most elegantly clear.
Tendons and ligaments share a fundamental vulnerability: they are hypovascular. The Achilles tendon, the rotator cuff, the patellar tendon — all of these structures have limited blood supply in their mid-substance, which is precisely where degeneration concentrates. Without adequate vascularity, the growth factors needed for repair cannot be delivered by the bloodstream in sufficient concentrations. The tissue degenerates silently, often painlessly at first, until enough fibres have failed that pain becomes unavoidable. By that point, the damage is extensive.
Injecting concentrated growth factors — particularly PDGF, TGF-β, VEGF, and FGF — directly into the degenerating tendon or its peritendinous sheath bypasses this vascular deficit entirely. VEGF stimulates new capillary formation, improving the baseline blood supply. PDGF activates tenocytes (tendon cells) and fibroblasts. TGF-β drives type I collagen synthesis — the structural collagen of tendons. FGF promotes cellular proliferation and matrix production. Together, these signals can shift a chronically degenerate, hypovascular tendon from a state of structural failure into active repair.
I want to speak plainly about something that I think is often glossed over in discussions of regenerative medicine: how you inject matters as much as what you inject.
Growth factor concentrates are expensive, biologically potent, and time-limited preparations. Injecting them even five or ten millimetres from the target tissue can reduce their biological effect dramatically. A growth factor concentrate injected into periarticular fat rather than the joint space, or into the paratenon rather than the tendon mid-substance, is not delivering its therapeutic payload where the damaged cells are. The preparation is wasted. The patient concludes the treatment failed. Often, it wasn't the biology — it was the placement.
At IBAP Clinics, every growth factor concentrate injection is performed under real-time ultrasound guidance. This is not a premium add-on. It is the standard of care that the biological preparation deserves. Ultrasound allows us to visualise the needle tip in real time, confirm intra-articular positioning with saline distension, identify and avoid neurovascular structures, and adjust trajectory dynamically during the procedure. For joint injections — particularly the hip, where surface anatomy is deeply unreliable — fluoroscopic or ultrasound guidance reduces injection accuracy error from approximately 30% (blind technique) to less than 2%.
20–90 ml blood drawn depending on preparation type. Processing takes 20 minutes (centrifuge-based) to 90 minutes (ACS incubation). Patient rests during preparation.
Diagnostic ultrasound of the target structure — joint, tendon, ligament — to confirm pathology location, identify optimal needle trajectory, and document baseline tissue appearance for follow-up comparison.
Sterile field preparation. Local anaesthetic to skin entry point — not to the target tissue, as this can alter the pH environment and potentially impair growth factor activity.
Fine-gauge needle advanced under continuous ultrasound visualisation. Position confirmed before injection. Growth factor concentrate delivered slowly to allow tissue distribution.
Activity restriction for 48 hours. Gentle range of motion from day 3. Structured physiotherapy programme commences at 1–2 weeks. Follow-up assessment at 4–6 weeks with repeat ultrasound where indicated.
If a clinic offers growth factor concentrate injections without real-time imaging guidance, please ask why. For superficial structures like the elbow epicondyle, experienced clinicians may achieve acceptable accuracy without imaging. For deep joints (hip, sacroiliac, facet), shoulder (glenohumeral), or intratendinous injections into small tendons, imaging guidance is not optional — it is the difference between a well-placed biological intervention and an expensive injection into the wrong tissue.
A detailed consultation with Dr Vijay Bhaskar will assess your imaging, clinical history, and disease stage to identify which biological preparation — if any — offers the best evidence for your specific condition.
2nd Floor, 284/A, Road No. 12,
above IDFC First Bank,
near Omega Hospitals, MLA Colony,
Banjara Hills, Hyderabad — 500034
Sy No. 2, 4th Floor, Plot No. 200,
beside South India Shopping Mall,
opp. Fortune Heights, Mythri Nagar,
Madeenaguda, Hyderabad — 500049
This article has been written by Dr Vijay Bhaskar Bandikatla for general informational and educational purposes only. It does not constitute medical advice, a clinical diagnosis, or a treatment recommendation for any individual. Growth factor concentrate therapies — including APS, ACS, plasma lysates, and related preparations — carry risks and benefits that must be evaluated on an individual basis by a qualified clinician following thorough clinical assessment and review of relevant imaging. The field of regenerative medicine is evolving rapidly; information reflects evidence available at time of publication. Not all preparations described are available in all clinical settings or regulatory contexts. Vijay Advanced Pain Clinics Pvt. Ltd. — Banjara Hills and Madeenaguda, Hyderabad.
EXCELLENTTrustindex verifies that the original source of the review is Google. Good pain relief with treatmentPosted on GoogleTrustindex verifies that the original source of the review is Google. Best for pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. बहुत अच्छा लगा हमें ये ट्रिटमेंट करा के अच्छे डॉक्टर और अच्छे स्टाफ हैं और काम पैसे में अच्छा अच्छा ट्रिटमेंट होता हैPosted on GoogleTrustindex verifies that the original source of the review is Google. Very nice, good and helpful staf, overall good experiencePosted on GoogleTrustindex verifies that the original source of the review is Google. Very good doctors and good tritment Thank you doctorPosted on GoogleTrustindex verifies that the original source of the review is Google. One of the best clinic for the relief of back painPosted on GoogleTrustindex verifies that the original source of the review is Google. Very good treatment indo british clinic for every pain reliefPosted on GoogleTrustindex verifies that the original source of the review is Google. I have visited indo british pain clinic this is superb clinic for pain relief that's why I have given 5 start rating to this clinic ...Posted on GoogleTrustindex verifies that the original source of the review is Google. My name is Raja Sekhar Reddy Tummuri from kakinada city My father was suffering nervous pain from last 3 years … I have decided to join with this op … Now everything fine after treatment done from DR. vijay sir … Wonderful service received from INDO British advanced pain clinic Hospitals in Hyderabad @ Banjara Hills road no 12.. Each and every staff response , concern , support & everything it’s too good Thank you so much … Special thanks to Mr. DR. Vijay bhaskar Bandi Katla …👏🏻👏🏻👏🏻👏🏻🙏🙏Verified by TrustindexTrustindex verified badge is the Universal Symbol of Trust. Only the greatest companies can get the verified badge who has a review score above 4.5, based on customer reviews over the past 12 months. Read more

Founder & Interventional Pain Specialist — IBAP Clinics, Hyderabad
MBBS · DA · FRCA (London) · FFPMRCA (Pain Medicine, UK) · MBA (Hospital Management)
CCT (Anaesthesia & Pain Medicine, UK) · Advanced Pain Training (Cambridge University Hospitals)
DDSMed Sports Medicine (Chicago) · Fellowship in Neuromodulation & Advanced Pain (London)
Dr Vijay brings over 15 years of postgraduate training across the United Kingdom’s most prestigious institutions — including the Royal College of Anaesthetists, Cambridge University Hospitals, and a dedicated neuromodulation fellowship in London — to his practice in Hyderabad. He is one of very few clinicians in India trained to the level of FFPMRCA — the Faculty of Pain Medicine of the Royal College of Anaesthetists — the highest qualification in pain medicine available in the UK.
His specialist expertise spans the full spectrum of knee pain management: from precision PRP and BMAC injections to cooled radiofrequency genicular nerve ablation, intrathecal drug delivery, and spinal cord stimulation for refractory pain states. He manages cases ranging from the weekend cricketer’s torn meniscus to the elderly cardiac patient with end-stage OA who has been told there are no further options.
Home » Procedures » Growth Factor Concentration

In our pain clinic, we provide pain relief so you can regain your identity.
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us