Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789

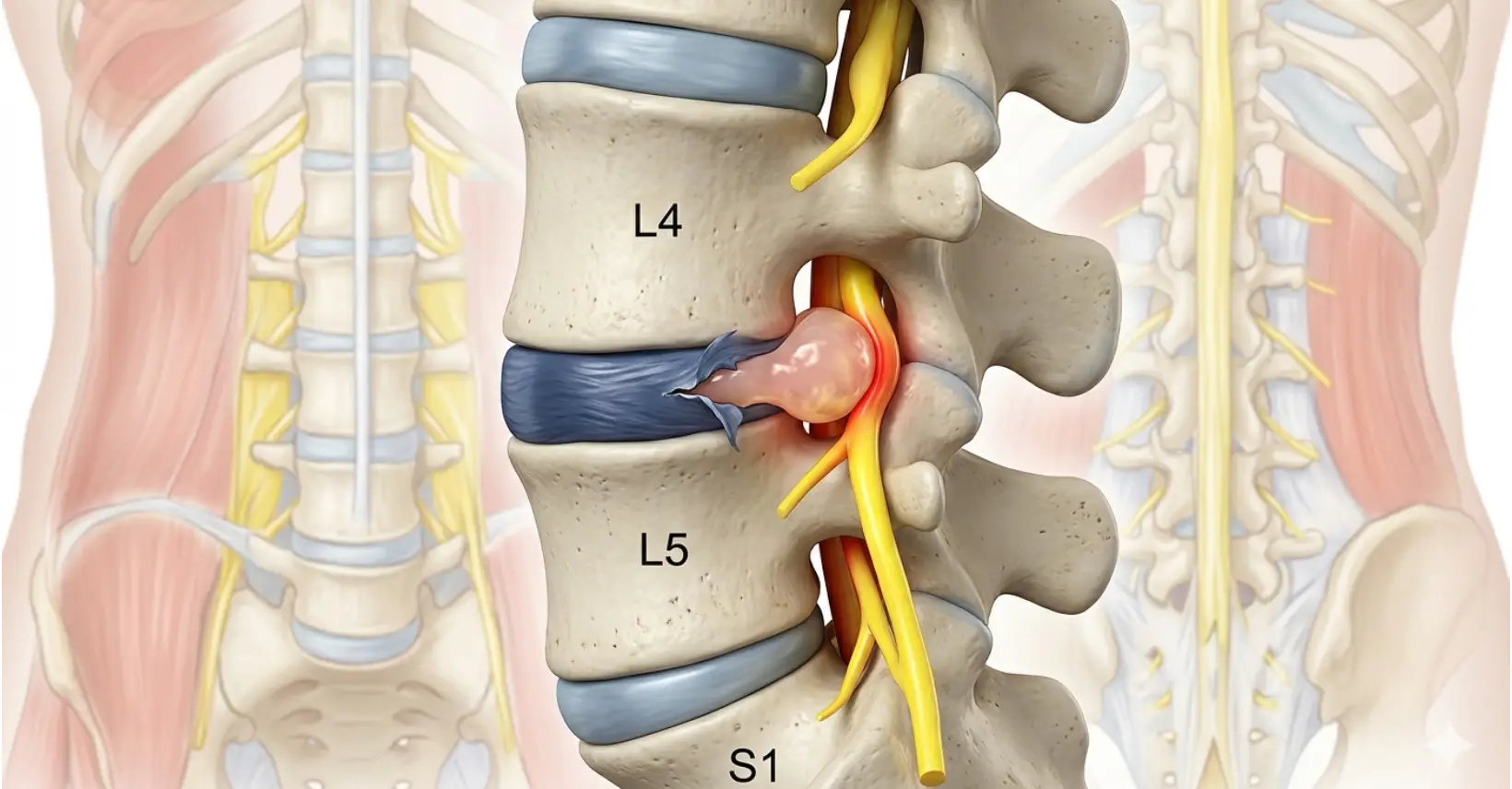
When the soft inner nucleus of a disc herniates through its outer ring, pressing on nearby nerve roots. Also called herniated disc, prolapsed disc or ruptured disc.
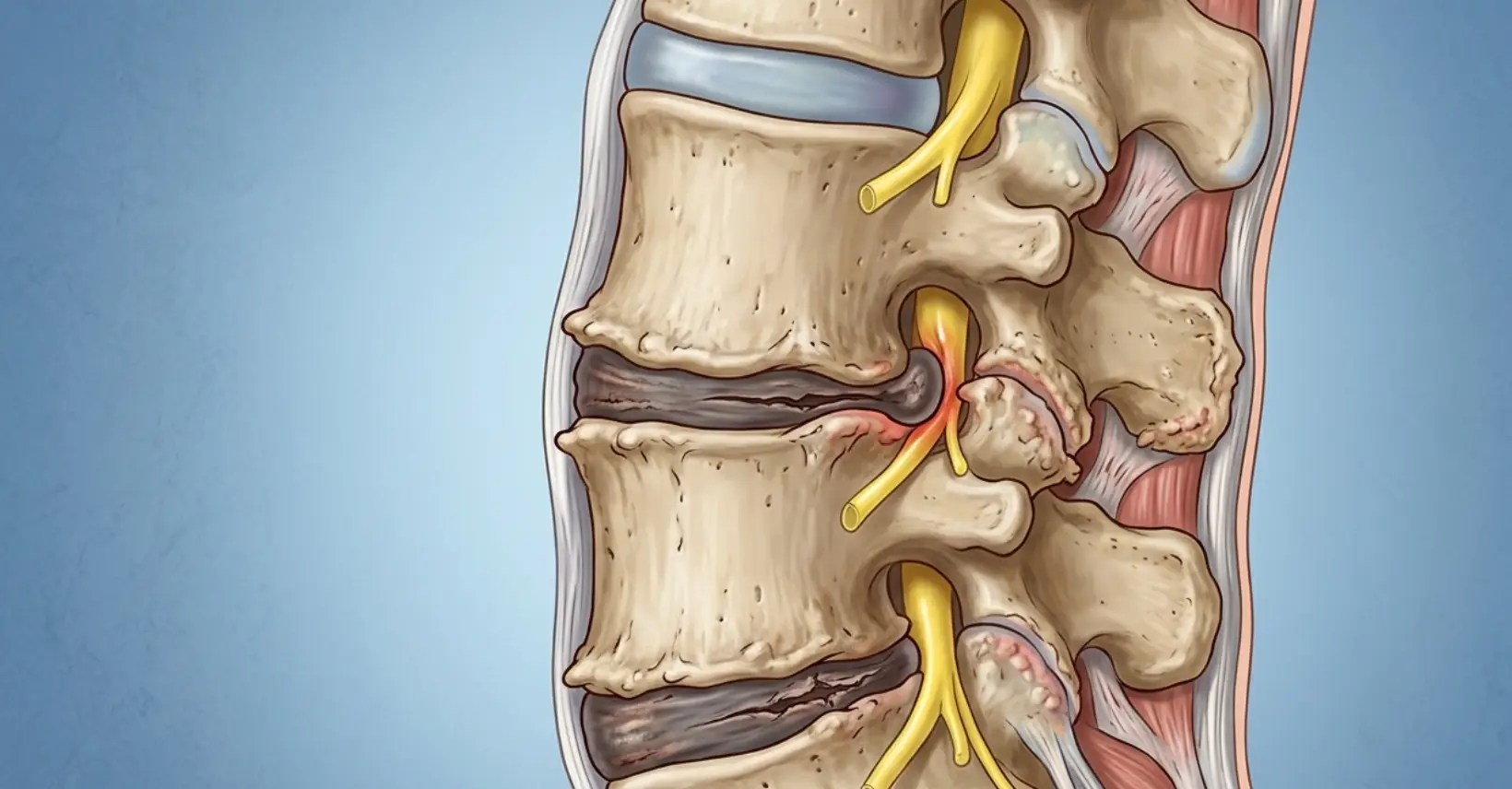
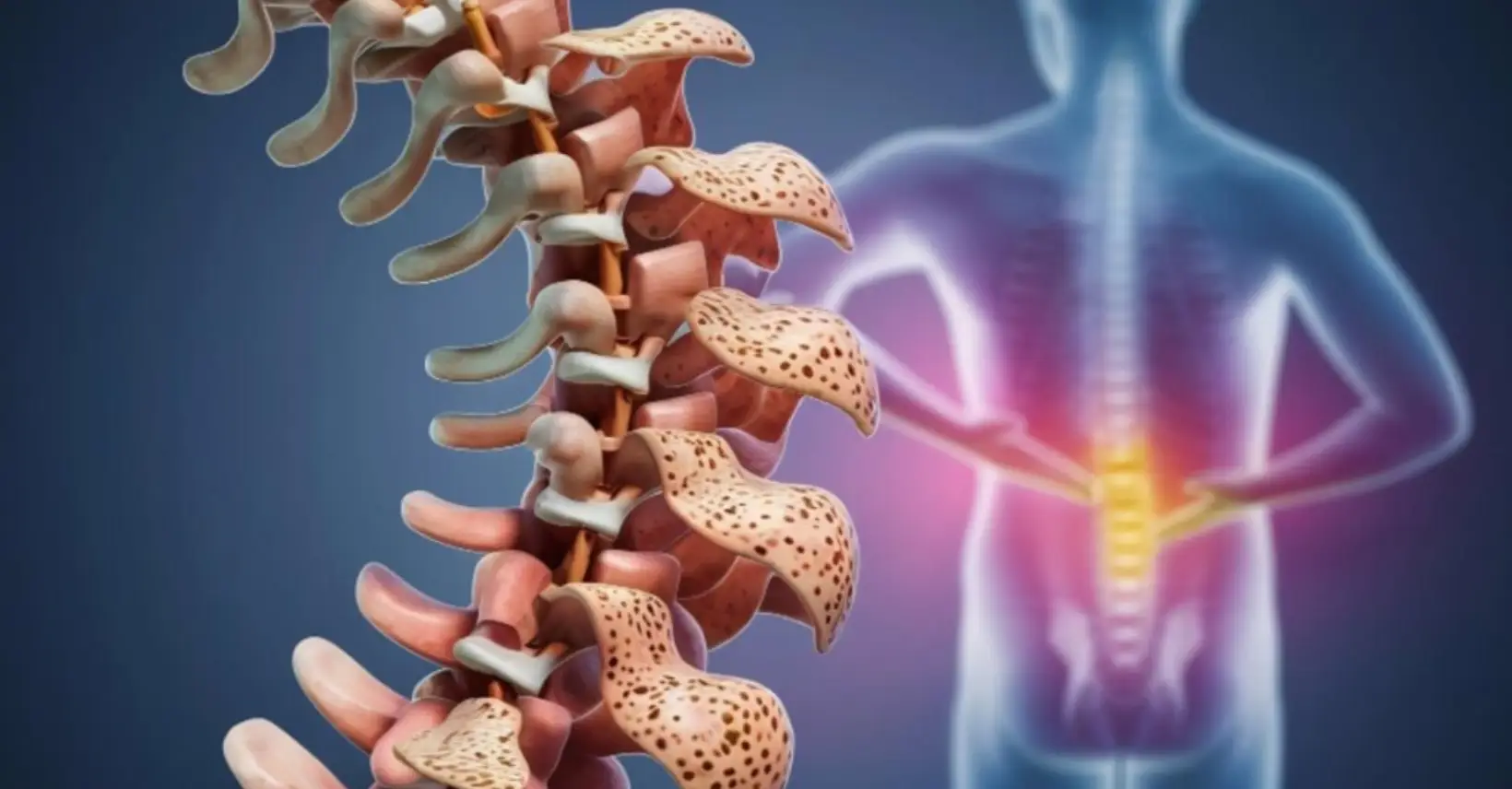
Age-related wear and tear of the discs, facet joints and vertebral end-plates. Disc degeneration occurs in over 80% of adults over the age of 50.
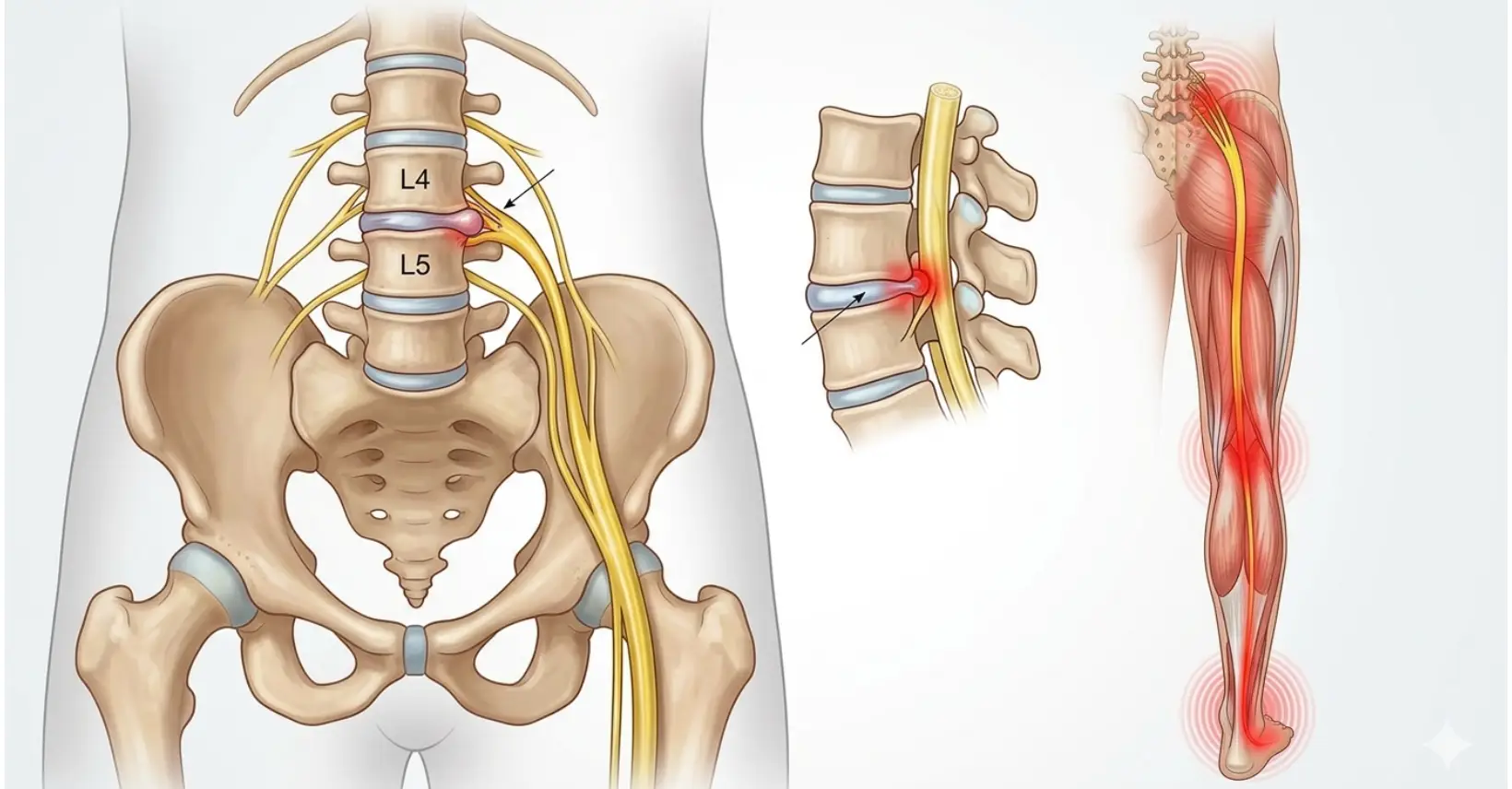
Compression or irritation of the sciatic nerve, causing pain, numbness or tingling to radiate from the lower back through the buttock and down the leg.
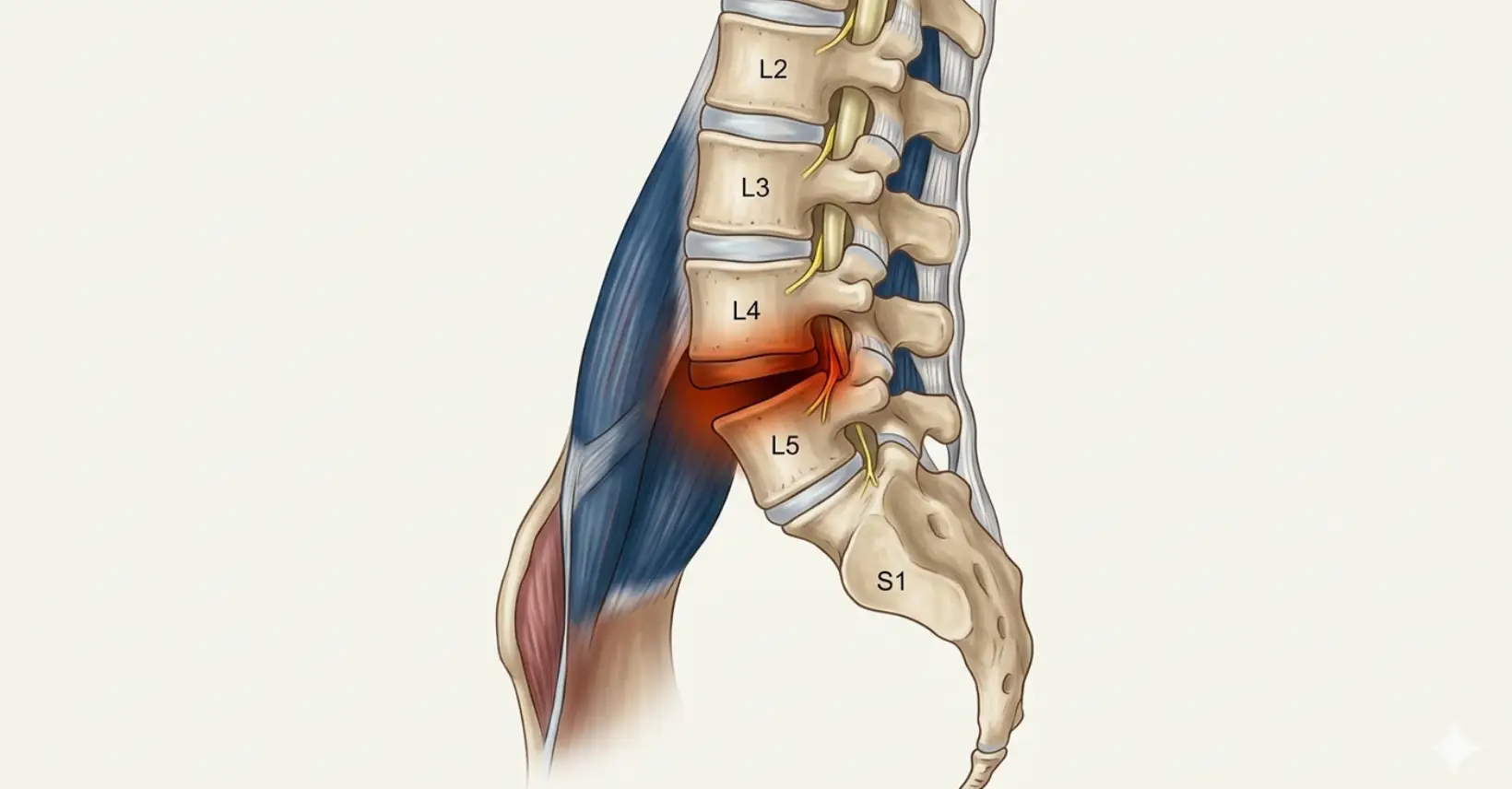
Forward slippage of one vertebra over another, most commonly at L4–L5 or L5–S1. Ranges from mild instability to significant nerve compression requiring intervention.

Inflammation of the vertebral joints — most notably Ankylosing Spondylitis (AS) and related spondyloarthropathies. Unlike mechanical back pain, spondylitis is immune-mediated and typically presents with early-morning stiffness lasting over 30 minutes, improving with activity rather than rest.
An older clinical term for non-specific low back pain. In modern pain medicine, lumbago is assessed to identify its structural cause rather than treated as a standalone diagnosis.

A thorough consultation exploring the nature, onset, character, radiation and aggravating factors of your pain. We use validated pain assessment tools alongside a functional disability evaluation.

Assessment of spinal mobility, nerve tension signs (straight leg raise, femoral stretch test), muscle strength, reflexes and sensory function to localise the pain generator.

Before proceeding to static imaging, we assess how your spine moves and loads. Digital Spinal Analysis (DSA) is a computerised, posture-based functional assessment that measures spinal alignment, range of motion, load distribution, and postural deviations in real time. Think of it as an ECG for your spine whereas X-ray or MRI shows structure, DSA shows function. It identifies compensatory patterns, muscle imbalances and biomechanical stress points that static imaging cannot reveal, allowing us to understand not just what is painful, but why it became painful and how to correct it.

Imaging is interpreted within the clinical context. Degenerative changes are common in asymptomatic adults — imaging findings alone do not determine treatment. MRI is the gold standard for soft tissue, disc and nerve assessment.

Targeted diagnostic nerve blocks — such as medial branch blocks or selective nerve root blocks — can confirm the pain source with precision before proceeding to definitive treatment.

Based on all the above, a tailored treatment pathway is designed — ranging from targeted injections and nerve blocks to radiofrequency ablation, regenerative therapies or neuromodulation for complex cases.

Targeted delivery of therapeutic agents to the precise pain source under fluoroscopic guidance

Energy-based denervation to interrupt pain signals — from conventional heat to cold and pulsed approaches

Minimally invasive treatments delivered directly into the disc — targeting the source of discogenic pain

Harnessing the body's own biology to repair, regenerate and reduce inflammation — moving beyond symptom suppression

Structural restoration of fractured or collapsed vertebrae — providing immediate pain relief and spinal stability

For complex, refractory or chronic pain where all other options have been exhausted
