Helpline :
9807 55 6789
-
Call Us Now: 9807 55 6789Call Us Now: 9807 55 6789
From the first twinge of osteoarthritis to a weekend footballer’s torn ACL – knee pain takes many forms. At IBAP Clinics, Hyderabad, our UK-trained interventional pain specialists map your exact diagnosis and craft a precision treatment plan: regenerative therapies, nerve ablation, and far more before surgery ever becomes necessary.

Click any spoke below to jump to that section of this comprehensive guide, or explore each dedicated article for deeper reading.

Foundation
Most Common

Autoimmune

Crystal Arthropathy

ACL · PCL · Meniscus
ACL, PCL, MCL, LCL
Soft Tissue
Periarticular

X-Ray · MRI · US · Blood

Regenerative · Ablation

Replacement · Osteotomy
Our Duty of Care
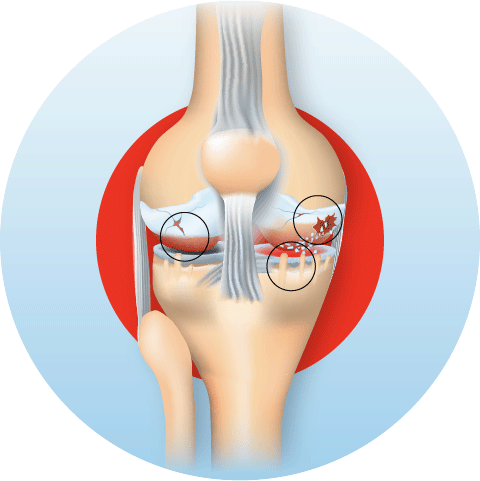
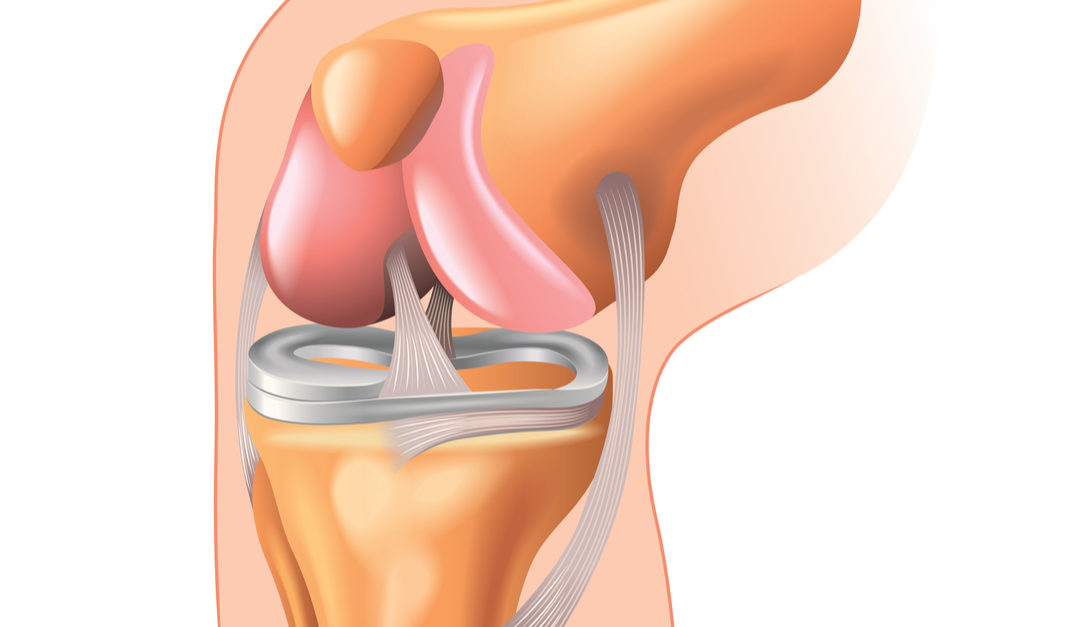
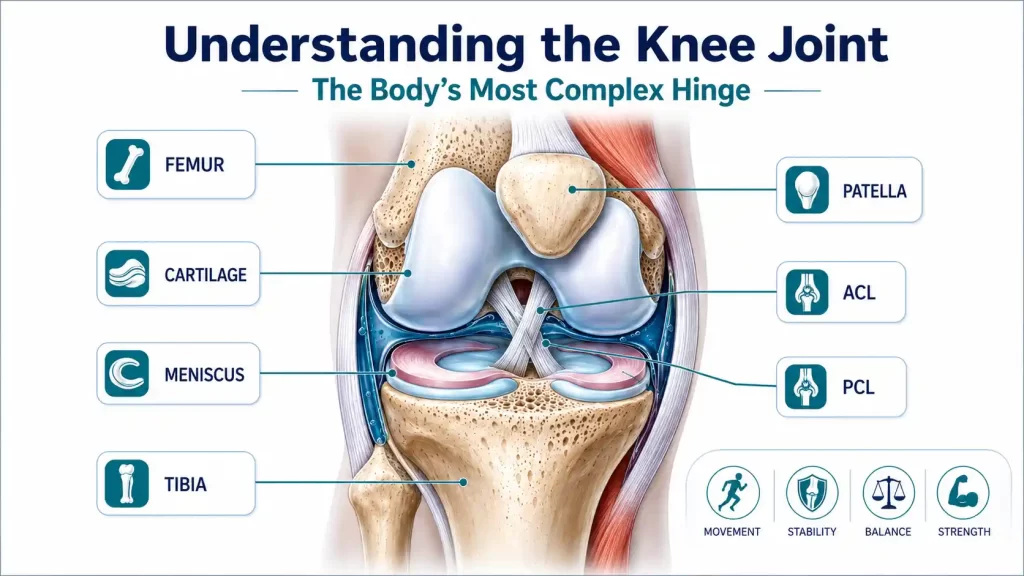
Think of your knee as the pivot of a suspension bridge: it bears the full weight of the body, absorbs ground-reaction forces during every step, and yet must rotate, flex, and straighten smoothly thousands of times a day. Unlike a simple door hinge, the knee combines three bones, four primary ligaments, two menisci, a bursa system, and the largest tendon in the body making it uniquely capable, and uniquely vulnerable.
The joint is formed where the femur (thigh bone) meets the tibia (shin bone), cushioned by the patella (kneecap). The joint surfaces are lined with hyaline cartilage a smooth, gel-like tissue that, once worn away, does not regenerate on its own. This is the root of most knee pain in adults.
💡
Did you know? The knee can experience forces up to 5–8× your body weight during activities such as climbing stairs or playing football — making it the most loaded joint in the body.
Osteoarthritis (OA) of the knee is the most prevalent joint disease worldwide and the leading cause of pain-related disability in adults over 50. Think of it as the natural wearing of a car tyre except the tyre cannot be replaced at a service station; it must be managed, preserved, and protected for life.
As the hyaline cartilage thins and erodes, bone rubs on bone, triggering pain, swelling, and the formation of bony spurs (osteophytes). The synovium becomes inflamed, producing excess joint fluid the familiar swollen, warm knee of a flare-up. Over time, the joint space narrows, and the leg may bow inward (varus) or outward (valgus) as the joint deforms.
Minimal osteophytes; mild symptoms. Responds well to lifestyle changes, physiotherapy, and PRP injections.
Definite osteophytes; slightly reduced joint space. Ideal window for regenerative therapies — PRP, hyaluronic acid, BMAC.
Significant cartilage loss; multiple osteophytes. Combination of BMAC, genicular nerve RFA, and bracing delivers best results.
Near-complete cartilage loss. Surgery may be considered, but for unsuitable patients, genicular RFA + BMAC remains highly effective for pain control.

⚠️
Risk Factors — Age over 50 · Obesity (every extra kg adds 4 kg of load on the knee) · Previous knee injury · Genetics · Occupational kneeling · Female sex (post-menopausal hormonal changes).
✅
IBAP Expertise: We specialise in managing early-to-moderate OA (KL Grades I–III) with disease-modifying regenerative therapies, aiming to delay or avoid surgery.
Rheumatoid arthritis (RA) is a systemic autoimmune disease in which the body’s immune system mistakenly attacks the synovial lining of joints. Unlike OA where cartilage wears away from mechanical overload RA inflames the synovium first, releasing enzymes that digest cartilage and bone from within. The analogy: OA is rust on a gate; RA is a fire inside the hinge.
The knee is frequently involved, presenting with warm, swollen joints, prolonged morning stiffness (>30 minutes), symmetric joint involvement, and constitutional symptoms such as fatigue and fever. Early diagnosis and disease-modifying anti-rheumatic drug (DMARD) therapy from a rheumatologist is paramount.

📋
Diagnosis Pointer: RA is confirmed by blood tests anti-CCP antibodies, Rheumatoid Factor (RF), raised CRP and ESR alongside characteristic MRI findings. At IBAP, we co-ordinate blood investigations and refer to rheumatology where needed.
Gout is caused by deposition of monosodium urate crystals within the joint, triggering one of medicine’s most excruciating pain attacks. Though classically affecting the big toe, the knee is the second most common site — particularly in older patients and those on diuretics. Pseudogout involves calcium pyrophosphate crystals and tends to target the knee preferentially.
Both conditions cause sudden, intense inflammatory arthritis — the knee becomes swollen, hot, and exquisitely tender, often waking the patient from sleep. An acute gout attack in the knee can mimic septic arthritis and demands urgent assessment.
Acute attacks are managed with targeted anti-inflammatory measures. Long-term management focuses on urate-lowering therapy (co-ordinated with the patient’s physician) and joint protection. For patients with chronic tophaceous gout causing structural knee damage, our interventional toolkit — including ultrasound-guided joint aspiration and injection — provides rapid, effective relief.
🩸
Key Blood Test: Serum uric acid. Levels >6 mg/dL in women and >7 mg/dL in men suggest hyperuricaemia — but levels may be paradoxically normal during an acute attack. Joint fluid analysis (polarised microscopy) remains the gold standard.
Whether it is a footballer’s pivot, a cricketer’s dive, or a runner’s repetitive stress — the knee bears the brunt of athletic endeavour. Understanding the specific structure injured is the first step to targeted recovery.
📏
A varus (outward) force injures the LCL and the complex posterolateral corner structures. These injuries are rarer but highly disabling — producing lateral instability and a “thrust” gait. The posterolateral corner requires specialist surgical management when severely disrupted.

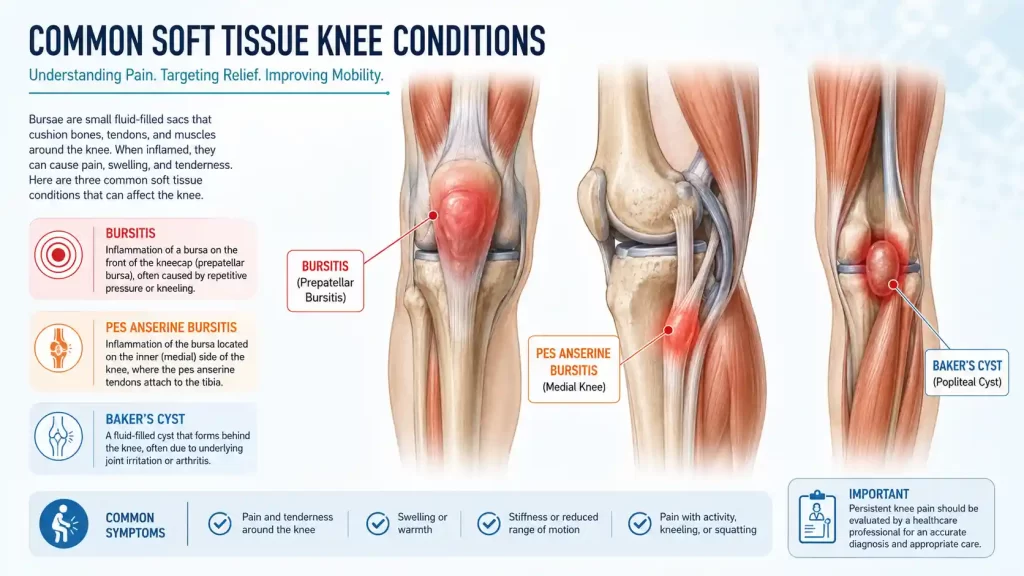
Bursae are small, fluid-filled sacs nature’s friction pads positioned between tendons, muscles, and bony prominences. The knee has over 13 bursae. When one becomes inflamed (bursitis), it produces localised pain, tenderness, and swelling that is distinct from intra-articular pathology.
Inflammation of the bursa in front of the patella caused by prolonged kneeling. Common in tilers, gardeners, and plumbers. The knee cap appears swollen, warm, and fluctuant. Usually responds to aspiration, padding, and a corticosteroid injection.
Often overlooked, this is inflammation of the bursa at the inner aspect of the upper shin — where the tendons of three muscles (sartorius, gracilis, semimembranosus) insert together, resembling a goose’s foot (pes anserine). It produces inner-knee pain worse at night and with stair climbing, commonly in overweight patients with OA. Ultrasound-guided injection with corticosteroid or PRP is highly effective and forms a core IBAP treatment.
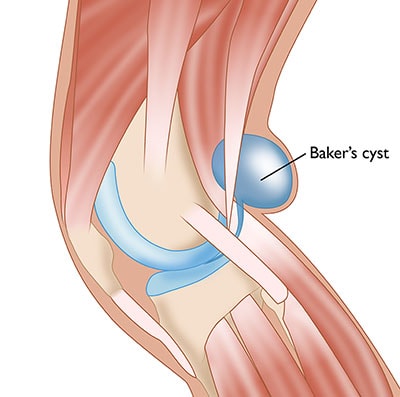
A Baker’s cyst is not a primary pathology — it is a secondary symptom. When the knee joint produces excess synovial fluid (in response to OA, meniscal tears, or RA), the fluid is pushed into the popliteal fossa (back of the knee) through a one-way valve in the joint capsule, forming a cyst. Treating the underlying cause — and aspirating the cyst under ultrasound guidance — resolves the problem definitively.
🎯
Pes Anserine Bursitis is a frequently missed diagnosis — particularly in diabetic patients and those with knee OA. If you have medial knee pain that is worse at night, ask us to check specifically for this condition.
⚠️
Caution: A ruptured Baker’s cyst can mimic a deep vein thrombosis (DVT) — causing sudden calf pain and swelling. Both conditions require urgent clinical assessment to distinguish them. IBAP Clinics uses ultrasound imaging to confirm the diagnosis at the point of care.
The patellar tendon connects the kneecap to the shin bone and is put under enormous stress during jumping, landing, and kicking. Repetitive overload causes degenerative changes (tendinosis) rather than true inflammation the tendon becomes thickened, disorganised, and painful. PRP injected precisely into the tendon under ultrasound guidance stimulates a healing response that physiotherapy alone cannot achieve.
Similar degenerative changes in the quadriceps tendon (above the patella) present as anterior knee pain, particularly in older athletes and individuals with a high BMI. Eccentric loading programmes combined with PRP or prolotherapy yield excellent results.
A friction syndrome causing lateral knee pain in runners the iliotibial band (a thick band of fascia running down the outer thigh) repeatedly rubs over the lateral femoral condyle. Ultrasound-guided injection at the point of impingement, combined with targeted hip strengthening, resolves the condition in most cases.
The popliteus muscle a small but vital stabiliser at the back of the knee can develop tendinosis, producing postero-lateral knee pain, often confused with a meniscal tear. Ultrasound assessment and targeted PRP injection are highly specific for this underdiagnosed condition.
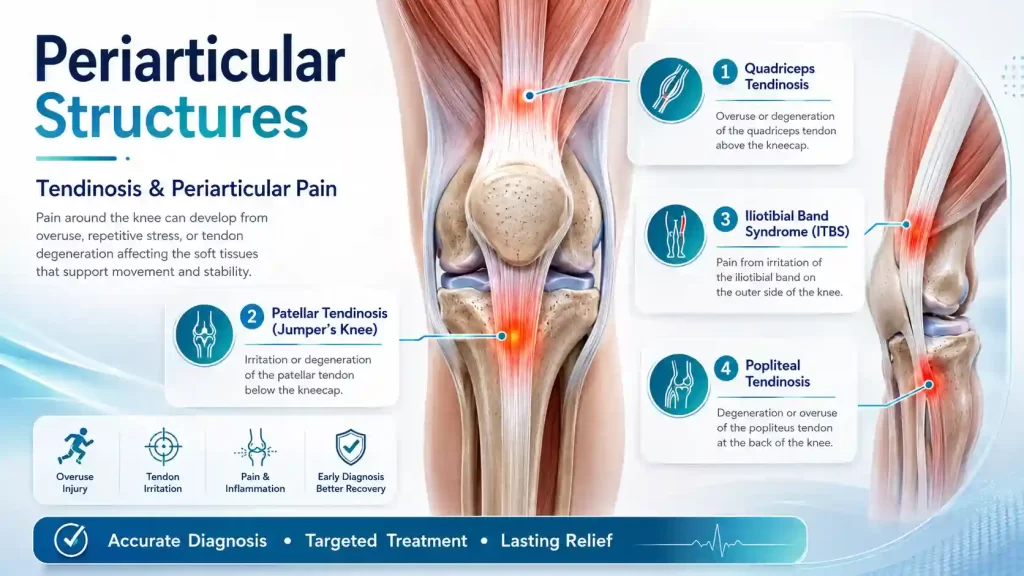
💡
Tendinosis vs Tendinitis: True inflammation (tendinitis) is short-lived. Most chronic tendon pain is actually tendinosis — degenerative disorganisation without inflammation. This distinction matters enormously because corticosteroids, which suppress inflammation, can weaken and even rupture a degenerated tendon. PRP and prolotherapy are therefore far safer and more effective long-term choices.
At IBAP Clinics, we believe that precision diagnosis is the foundation of precision treatment. Our diagnostic pathway is a stepwise, evidence-based process starting with a thorough clinical history and examination, and adding investigations judiciously. We never treat an X-ray; we treat a person.
🩻
The first-line investigation for any knee pain. Standing (weight-bearing) films accurately measure joint space narrowing, osteophyte formation, and deformity (varus/valgus). Used to grade OA using the Kellgren–Lawrence scale and guide surgical planning.
🩺
IBAP’s dynamic, real-time imaging tool. Ultrasound identifies effusions, bursitis (prepatellar, pes anserine), Baker’s cysts, tendon tears, soft tissue masses, and nerve pathology — all at the point of care in clinic. Also used to guide injections with pinpoint accuracy.
🔬
The gold standard for soft tissue assessment. MRI delineates meniscal tears (pattern and grade), cruciate and collateral ligament integrity, cartilage thickness, bone marrow oedema, and popliteal pathology. Essential for surgical planning and for assessing suitability for regenerative therapies.
🩸
Requested selectively when inflammatory, autoimmune, or metabolic causes are suspected. Panel typically includes: CRP, ESR, Full Blood Count, Rheumatoid Factor, anti-CCP antibodies, Uric Acid, and HLA-B27. Results integrate with imaging for a complete picture.

🎯
The IBAP Approach: Every investigation at IBAP Clinics is interpreted in the context of your symptoms, examination findings, and life circumstances — not in isolation. A “mildly arthritic” X-ray in a 45-year-old marathon runner represents a vastly different clinical challenge to the same finding in an 80-year-old with multiple comorbidities.
At IBAP Clinics, we build a personalised, stepped treatment plan — starting with the least invasive, most effective option and escalating thoughtfully. Our treatments range from lifestyle optimisation and physiotherapy to the most advanced regenerative biologic injections and neuromodulatory techniques available anywhere in India.
PRP is your own blood, concentrated to 5–7× its normal platelet count. Platelets release growth factors — PDGF, TGF-β, VEGF — that orchestrate tissue repair. Think of PRP as applying a concentrated repair crew directly to damaged cartilage and tendons.
BMAC is harvested from the patient’s own iliac crest (hip bone), concentrated, and injected into the knee. It contains mesenchymal stem cells, growth factors, and anti-inflammatory cytokines — the most potent autologous (self-sourced) biological therapy available for joint disease.
⚡
The genicular nerves are small sensory branches that carry pain signals from the knee to the brain — without contributing to movement. CRF ablation applies controlled heat to these nerves, interrupting the pain pathway while leaving motor function entirely intact. It is the most powerful non-surgical pain intervention for moderate-to-severe knee OA.
Hyaluronic acid (HA) is a naturally occurring polymer in healthy joint fluid — the “engine oil” of the knee. In OA, HA becomes denatured and loses its lubricating and shock-absorbing properties. Injecting high-molecular-weight HA restores the joint’s viscoelastic environment, reducing friction and pain.
Prolotherapy involves injection of a mildly irritant solution (typically hypertonic dextrose) into degenerated ligaments, tendons, and joint spaces. This controlled irritation triggers a localised inflammatory healing cascade — producing collagen synthesis and strengthening of lax or degenerated structures. An elegant analogy: “teaching the body to repair what it had forgotten was broken.”
Corticosteroid (CS) injections remain a valuable, rapid-acting tool for acute inflammatory flares — RA exacerbations, acute bursitis, gout attacks, and post-surgical inflammation. At IBAP, we use them selectively and sparingly, as repeated CS injections accelerate cartilage loss and should never be used as routine OA management.
No injection or procedure works in isolation. Physiotherapy strengthens the muscles that support and off-load the knee joint — quadriceps, hamstrings, hip abductors, and core — reducing mechanical stress and preventing recurrence. At IBAP, we prescribe structured, evidence-based rehabilitation protocols aligned to each patient’s diagnosis, age, and functional goals.

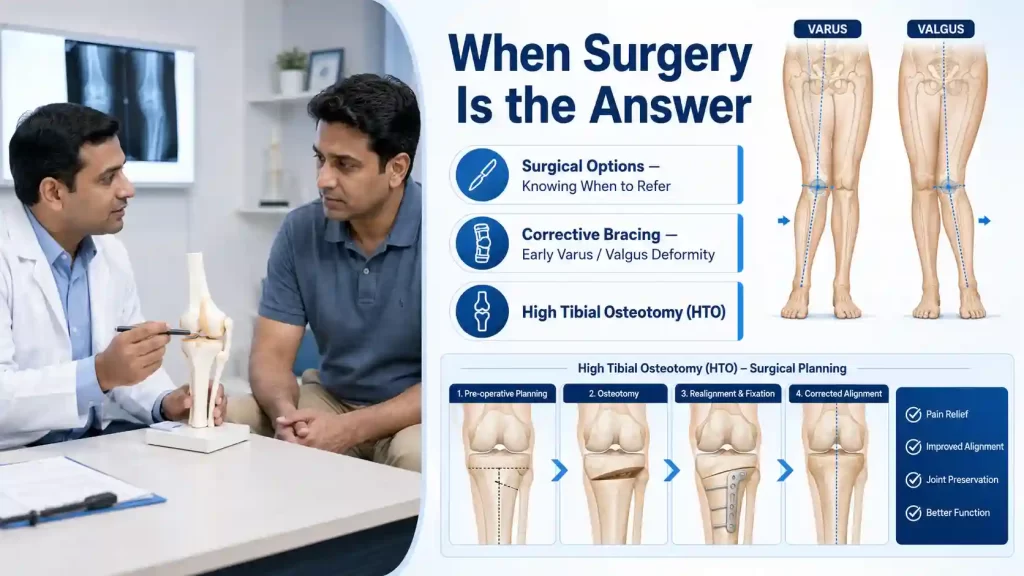
IBAP Clinics is not an anti-surgery practice we are a pro-appropriate-surgery practice. Our expertise lies in ensuring that patients receive the right intervention at the right time. Surgery is the correct answer for certain patients at certain stages and our role is to get them there in the best possible condition, or to delay that time as long as is clinically safe and patient-appropriate.
When KL Grade II–III OA is accompanied by early varus (“bow-leg”) or valgus (“knock-knee”) deformity, an offloading knee brace can shift mechanical load away from the damaged compartment, slowing disease progression and reducing pain. IBAP co-ordinates specialist brace prescription and review as part of the conservative management plan.
In younger, active patients with unicompartmental (one-sided) OA and significant varus or valgus malalignment, a high tibial osteotomy surgically realigns the leg — redistributing weight to the healthier cartilage compartment. This buys 10–15 years before a potential replacement is needed, and is the ideal surgical option for patients aged 35–55.
For end-stage OA (KL Grade IV) with bone-on-bone contact, significant deformity, and failure of all conservative treatments, total knee arthroplasty (TKA) or unicompartmental knee replacement (UKR) restores anatomy and dramatically improves quality of life. Surgical outcomes are now excellent modern implants have a 95% 15-year survival rate.
🤝
Our Surgical Referral Network: IBAP Clinics maintains collaborative relationships with leading orthopaedic surgeons in Hyderabad. When surgery is indicated, we provide a warm referral with full clinical documentation and continue to manage the patient’s pain perioperatively and postoperatively.
There is a category of patient that the surgical world often struggles to help — and yet whose need for pain relief is the most urgent and the most human. These are the patients for whom surgery carries too great a risk, or for whom it is simply not a viable path:
Evidence-based answers from Dr Vijay Bhaskar, Interventional Pain Specialist, IBAP Clinics, Hyderabad.
Yes the majority of knee pain conditions, including mild-to-moderate osteoarthritis, tendinosis, bursitis, ligament sprains, and inflammatory arthritis, can be effectively managed without surgery. At IBAP Clinics, we employ a comprehensive non-surgical toolkit including PRP, BMAC (stem cell therapy), hyaluronic acid injections, genicular nerve radiofrequency ablation, prolotherapy, and structured physiotherapy rehabilitation. Even in advanced OA (KL Grade IV), where the patient is unfit for surgery, genicular nerve CRF ablation can provide 6–24 months of significant pain relief.
Platelet-Rich Plasma (PRP) is a concentrate of your own blood, processed to contain 5–7× the normal platelet count. Platelets release a rich cocktail of growth factors (PDGF, TGF-β, VEGF) that stimulate cartilage repair, tendon healing, and suppression of inflammation. A course of three weekly ultrasound-guided PRP injections has been shown in multiple RCTs and meta-analyses to significantly reduce knee pain and improve function in osteoarthritis grades I–III outperforming both hyaluronic acid and corticosteroids at 6–12 month follow-up. The ESSKA ORBIT 2024 consensus supports its use in early-to-moderate OA.
Genicular nerve radiofrequency ablation (GnRFA) is a minimally invasive procedure that applies controlled radiofrequency energy to the small sensory nerves around the knee — the genicular nerves — interrupting the pain signal without affecting leg movement. It is performed as a day procedure under local anaesthetic, requiring no general anaesthesia or hospitalisation. GnRFA is suitable for patients with moderate-to-severe knee OA (KL Grades III–IV) who have failed conservative treatments, patients with pain persisting after knee replacement, and patients who are medically unfit for surgery. Pain relief typically lasts 6–24 months and the procedure can be safely repeated.
Distinguishing between different causes of knee pain requires a combination of clinical history, physical examination, and targeted investigations. Osteoarthritis typically presents with gradual-onset pain in patients over 50, worsened by activity and relieved by rest, with morning stiffness lasting less than 30 minutes. Rheumatoid arthritis causes prolonged morning stiffness, symmetric joint involvement, and systemic symptoms. Meniscal tears produce joint-line tenderness, locking, and a history of twisting injury. Bursitis presents as localised tenderness over the bursa with preserved joint movement. At IBAP Clinics, we use X-ray, ultrasound, MRI, and blood tests in a structured diagnostic pathway to reach an accurate diagnosis — because treatment effectiveness depends entirely on treating the correct condition.
BMAC (Bone Marrow Aspirate Concentrate) is an autologous therapy — derived entirely from the patient’s own bone marrow — making it inherently biocompatible with a very favourable safety profile. Multiple prospective clinical trials and RCTs have confirmed its safety in knee OA. A 4-year follow-up study published in Scientific Reports (2024) demonstrated sustained improvement in WOMAC and IKDC scores in KL Grade III–IV OA with no significant adverse events. At IBAP Clinics, BMAC is harvested under sterile conditions and injected under imaging guidance — maximising both safety and effectiveness.
In most cases, no. A Baker’s cyst (popliteal cyst) is a secondary problem caused by excess fluid in the knee joint — typically from osteoarthritis, a meniscal tear, or inflammatory arthritis. Surgically removing the cyst without treating the underlying cause invariably leads to recurrence. At IBAP Clinics, we first identify and treat the root cause (e.g., PRP or BMAC for OA, HA injection, or anti-inflammatory management for RA). The cyst can then be aspirated under ultrasound guidance and, if necessary, a corticosteroid or hyaluronic acid injection administered. Surgery is very rarely required for an isolated Baker’s cyst.
A great deal can be achieved, and at IBAP Clinics we are specifically experienced in managing patients who cannot undergo surgery — whether due to advanced age, recent cardiac events, kidney disease, active cancer, or other comorbidities. Our non-surgical options include: genicular nerve CRF ablation (performed under local anaesthetic only), intra-articular BMAC or PRP injections, hyaluronic acid viscosupplementation, targeted corticosteroid injections for inflammatory flares, and optimised pain medications. Each plan is individualised, compassion-led, and focused on maximising quality of life and functional independence.

Founder & Interventional Pain Specialist – IBAP Clinics, Hyderabad
MBBS · DA · FRCA (London) · FFPMRCA (Pain Medicine, UK) · MBA (Hospital Management)
CCT (Anaesthesia & Pain Medicine, UK) · Advanced Pain Training (Cambridge University Hospitals)
DDSMed Sports Medicine (Chicago) · Fellowship in Neuromodulation & Advanced Pain (London)
Dr Vijay brings over 15 years of postgraduate training across the United Kingdom’s most prestigious institutions – including the Royal College of Anaesthetists, Cambridge University Hospitals, and a dedicated neuromodulation fellowship in London – to his practice in Hyderabad. He is one of very few clinicians in India trained to the level of FFPMRCA – the Faculty of Pain Medicine of the Royal College of Anaesthetists – the highest qualification in pain medicine available in the UK.
His specialist expertise spans the full spectrum of knee pain management: from precision PRP and BMAC injections to cooled radiofrequency genicular nerve ablation, intrathecal drug delivery, and spinal cord stimulation for refractory pain states. He manages cases ranging from the weekend cricketer’s torn meniscus to the elderly cardiac patient with end-stage OA who has been told there are no further options.
Banjara Hills
2nd Floor, 284/A, Road No. 12, above IDFC First Bank, near Omega hospitals, MLA Colony, Banjara Hills, Hyderabad, Telangana 500034.

Indo-British Advanced Pain Clinic © 2026. All Rights Reserved. Designed & Developed By Adroit
WhatsApp us